Download

1 / 44
450 likes | 795 Views
Latent TB infection . Dr CC Leung TB & Chest Service Public Health Services Branch Centre for Health Protection Department of Health 香港特別行政區 衞 生署 衞 生防護中心胸肺科. 香港地理及人口. 中國大陸之南部 人口數目 = ~6,800,000 土地面積 = 1098 平方公里 人口密度 = 每平方公里 ~6500 人. 香港的醫療系統. 公營 私營 基層醫療服務 30% 70%

E N D
Latent TB infection Dr CC Leung TB & Chest ServicePublic Health Services BranchCentre for Health ProtectionDepartment of Health香港特別行政區衞生署 衞生防護中心胸肺科
香港地理及人口 • 中國大陸之南部 • 人口數目 = ~6,800,000 • 土地面積 = 1098 平方公里 • 人口密度 = 每平方公里~6500人
香港的醫療系統 公營 私營 基層醫療服務 30% 70% 醫院服務 90% 10%
香港診治結核病之服務 結核病患者 衞生署 胸肺診所 19 間診所 每年約6,000 症 衞生署 普通科 門診部 醫管局 急症部 基層 私家醫生 醫管局胸肺醫院 主要有5 間醫院 約800 病床 7,000 住院人次 私家醫院 醫管局 專科門診 醫管局 一般醫院 第二層
LTBI: Screen and Treat ? • Disease • Natural History / Impact • Diagnostic / Treatment Tools • Effectiveness / Limitations • Goal of Intervention • Personal protection / Public health control • Cost-effectiveness • Individual level / Community perspective
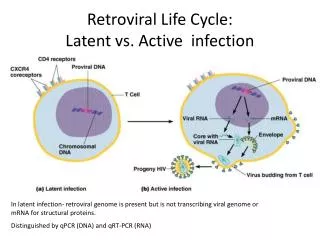
Latent TB Infection • Infection by the tubercle bacillus is pre-requisite for development of disease • Latent Period • Long and Variable • Asymptomatic and Non-infectious • Provide an opportunity for intervention
From Infection to Disease • Risk of developing disease • Multiple factors related to interaction between pathogen and human host • Lifetime Risk: • About one in ten (average) • The risk is greater initially • 5% within initial 2-5 years • 5% during the rest of lifetime
Predisposing Conditions • HIV infection • Steriod / Immunosuppresant / anti-TNF • Silicosis • Chronic Renal Failure / hemodialysis • Diabetes Mellitus • Underweight • Gastrectomy / Jejunoileal Bypass • Malignancy / Debilitated State • Alcoholism / Smoking / Injection Drug Use
Active TB Disease - 2003 WHO Fact sheet N°104 (Revised April 2005)
Can we wait until disease ? • Airborne spread • major challenge in control • Nonspecific symptoms • delay in diagnosis • Serious forms • grave consequences • High bacilli load • mutation and resistance
Diagnostic tools • Traditional standard • Tuberculin test • Newer interferon-γrelease test • T Spot-TB®(Oxford Immunotec) • QuantiFERON®-TB Gold (Cellestis)
Tuberculin test • Intradermal injection preferred for better standardization • 2 units of PPD-RT23 (equivalent to 5 units of PPD-S)
Largest transverse diameter of induration read between 48-72 h
Specificity (TST) • PPD contains a mixture of proteins • not entirely specific to the tubercle bacillus • potential cross-reactivity with other mycobacterial species • Positive reaction can occur with: • Active disease / Latent Infection • BCG vaccination / Booster • Other mycobacterial species
BCG Vaccination(HK) • BCG vaccination • First introduced in April 1952 • Neonatal vaccination • 99% coverage since 1970’s • Revaccination • Stopped only in 2000
Sensitivity (TST) • Exact sensitivity for latent TB infection uncertain in absence of gold standard • Around 80%-90% sensitivity in active TB cases, • Varies with strength of tuberculin / cut-off point • Trade-off between sensitivity and specificity • False negative can also occur with a number of other conditions
Interferon-γRelease Test • Earlier version: • Measures the production of interferon- (IFN-) in T-lymphocytes upon stimulation with PPD. • Newer assays: • PPD is replaced by ESAT-6 and CFP10 (specific for MTB and not present in BCG and most MOTT)
QuantiFERON® -TB Gold • Whole blood assay • Stimulate lymphocytes • in fresh whole blood • with ESAT-6 and CFP10 • Measure IFN- level by • Enzyme-linked immunosorbent assay • Cell isolation not required • Variable background response: • Cut-off value may not be too sharp • Approved by FDA, USA in May 2005
T Spot-TB® • ELISPOT test • Isolation of lymphocytes from fresh blood • Incubation with ESAT-6 and CFP10 • Enzyme-Linked ImmunoSPOT assay • For INF--producing T-lymphocytes • More tedious, but may be more sensitive • Approved for use in Europe
Sensitivity and Specificity • Estimation is difficult • No gold standard for latent TB infection • Estimate of Sensitivity • positive rate in bacteriologically confirmed TB • 45/47 (Elispot, Lavani 2001) • Estimate of specificity • negative rate in BCG vaccinated subjects without risk factor for exposure • 26/26(Elispot, Lavani 2001) Lavani et al, Lancet 2001;23:2017-21
ELISPOT vs TST(School Outbreak, UK) • Good Agreement • 89% concordance, kappa=0·72, p<0·0001 • ELISPOT correlated better with • proximity (p=0·03) • duration of exposure (p=0·007) • TST more likely to be positive • in BCG-vaccinated vs unvaccinated (p=0·002) • ELISPOT results • Not associated with BCG vaccination (p=0·44). Ewer K, et al. Lancet 2003; 361: 1168–73
Potential advantages • Higher sensitivity • ?Help rule out infection / disease • More specific (specific antigens) • ?Help to rule in infection / disease • No booster effect on repeated testing • Good for serial surveillance • One clinic visit instead of two: • May facilitate uptake
Limitations • Require prompt delivery of fresh blood • Technically much more demanding • Currently much more expensive • Test for infection rather than disease • Clinical experience is limited at this stage • Changes with time after exposure and treatment • Not fully evaluated in terms of the risk of disease development
Treatment of LTBI • Single drugs or simple combinations of two drugs • Isoniazid for 6 to 12 months • 5mg/kg daily (maximum 300mg) • 15mg twice weekly (maximum 900mg) (US) • Alternative regimens • Rifampicin for 4 months (US) • Isonoazid and Rifampicin for 3 months (Europe)
Hepatotoxicity • Notwithstanding the use of only one or two drugs, hepatotoxicity remains an important side effect • While untreated active TB often kills, only one out of ten latently infected subjects will actually develop disease. • Caution is therefore required in subjecting these asymptomatic individuals to treatment.
Possible Approaches • Population Approach: • All infected individuals within the community • Targeted Approach: • High risk of Disease / Grave Consequence
Factors for Consideration • Goal of intervention • Personal Protection / Public Health Control • Cost-effectiveness • Prevalence of infection / Risk of Disease • Limitations of Diagnostic / Treatment Tools
Reactivation vs Recent Transmission TB cases Progressive primary * Exogenous reinfection * Endogenous reactivation # 1950 2000 Year Ageing of the TB epidemic
Aging of the TB Epidemic • Population-based IS6110-based RFLP study • 24.5% (of 691 isolates) belonged to clusters • Recent transmission: 15 to 20% • Endogenous reactivation • Treat active disease by DOTS • Control recent transmission But • Little impact on endogenous reactivation Chan-Yeung M, et al. J Clin Microb 2003;41:2706-8
Population Approach • Treatment of latent TB reduces endogenous reactivation • Can we treat every infected one to eliminate TB from our population?
Estimated Infection Rate (HK) *Estimation based on: Incidence (smear-positive cases) = ARI * Styblo ratio
Number to Treat ( HK Primary Students) Leung CC et al. Risk of TB among school children in Hong Kong. Arch Ped Adol Med, in press
Targetted Approach (HK) • High-risk groups: • Recent Contacts • HIV • Silicosis • Immunosuppressive Treatment / Anti-TNF
Recent vs Remote Infection • Remote infection • Much lower risk of disease • Increases with age • Interferon-γrelease test • More specific BUT • May not differentiate between recent and remote Infection
Predictive Value of Positive Testfor Recent Infection / Reinfection Assume: 100% sensitivity & specificity; 20% recent transmission
Targetted Approach: Impact • Personal protection • More cost-effective than population approach • Limited Impact on TB control • Prevent few cases, e.g. Close contacts • Initial screening: • Only 2% of all notifications locally • Not directly preventable as already disease • Later 5 years: only another 4% at best
Looking into Future • Researches and Development: • Better characterization of disease risk • Newer diagnostic tools • Simpler, and more affordable • Better ability to predict actual disease risk • Better treatment regimen • Shorter, safer and more effective • Affordable and Acceptable for wide application