Download
1 / 30
300 likes | 328 Views
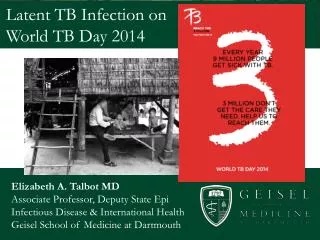
Latent TB Infection Sarah Mungall Bristol Royal Infirmary 1 st March 2018. Figure 1.4. Three-year average tuberculosis case rates by local areas*, UK, 2009-2011. *England – Local Authorities, Scotland – NHS Boards, Wales – Local Health Boards, NI – data not available.

E N D
Latent TB Infection Sarah Mungall Bristol Royal Infirmary 1st March 2018
Figure 1.4. Three-year average tuberculosis case rates by local areas*, UK, 2009-2011 *England – Local Authorities, Scotland – NHS Boards, Wales – Local Health Boards, NI – data not available. Sources: Tuberculosis in the UK: Annual report on tuberculosis surveillance in the UK, 2012. London: Health Protection Agency. July 2012. 5th July 2012
Background • Who to screen • How to screen • Who to screen • How to treat
UK versus US - the situation (>)5 years ago • TB rates halved in white US born citizens in US in last 10 years • No decline in TB cases in white UK born citizens in last 10 years
Collaborative TB Strategy2015 - 2020 Improve access to services and ensure early diagnosis Provide universal access to high quality diagnostics Improve treatment and care services Ensure comprehensive contact tracing Improve BCG Vaccination uptake Reduce drug-resistant TB Tackle TB in under-served populations Systematically implement new entrant latent TB (LTBI)screening Strengthen surveillance and monitoring Ensure an appropriate workforce to deliver TB control
Screening for latent TB infection • TB contacts • Occupational Health • PHE new entrant latent TB pilot • Prior to biological therapy
Contact tracing • All household contacts if pulmonary disease • All household contacts and casual contacts if smear positive pulmonary disease • (NICE guidance 2016) • “Inform and advise”
Contact tracing • Screen symptomatic contacts immediately • Asymptomatic – screen at 6-12 weeks • >65 symptoms and CXR • <65 symptoms and 1 or 2 step test (ie screen for latent TB infection) • 1 step test – IGRA • 2 step test – TST and IGRA
Metanalysis of IGRA sensitivity/ specificity-mean resultsMenzies D et al Ann. Int. Med 2007
Occupational Health • If recently arrived from high incidence country • If >3 months in high incidence country
Latent TB Pilot • For areas with an incidence of TB of >20/100,000 • GPs to do IGRA for patients aged 16-35 recently arrived from high incidence country (>150/100,000) • Refer to secondary care if positive IGRA
Biological Therapy • BTS guidelines 2005 are complicated! • Don’t include role of IGRA
How do we screen for latent TB infection? • Quantiferon TB Gold Interferon Gamma Release Assay ( IGRA) • T Spot TB IGRA
How do we screen for latent TB infection? • If immuncompromised screening more complicated • If HIV infection latent disease reactivation risk is 50 – 100 times higher (5% per year)
Recruited 120 liver transplants, 116 HIV and 95 Haematological malignancies and performed simultaneous Mantoux, Quantiferon and Tspot tests Overall results:- Tuberculin test 10.9% + T spot 18.4% + Quantiferon 15.1% + At least 1 test positive:- HIV 9.5% Haematological malignancies 29.5% Liver transplant 35.8% How reliable is IGRA in immunocompromised patients?Richeldi L et al Chest 2009
201 HIV+ patients had Ellispot, then monitored for 2 years 154 with history/ radiology suggesting active/ probable TB Sensitivity 90.3%, specificity 100%, negative predictive value 98.2% Poor correlation with CD4 count, (although only 18% had counts <100 cells/ μl) -but patients with active TB had significantly lower mean count than those with latent TB 47 screened for latent disease: 20 were IGRA+ 2 developed active TB within next 10 months TB ELISPOT IN HIVClark S et al, Clinical & Experimental Immunology 2007;1365
Principle of IGRAs • Specific antigens for M TB, M Africanum & M Bovis • Not present in BCG • Only found in a few atypical species:- • M Kansasii • M Marinum • M Szulgai
Whole Blood IFN- AssayQuantiFERON-TB Test Stage 1 Whole Blood Culture Nil Control Mitogen Control ESAT-6 CFP 10 Incubate → INF- from sensitized T-cells Aliquot blood & add antigen Draw blood + heparin Stage 2 IFN-gamma ELISA COLOR TMB Computerized interpretation Harvest plasma from above settled cells Measure [ IFN-g ] in ‘Sandwich’ ELISA Cellestis
T-Spot.TB: “Sixeasy Steps” Nil Control Infection Infection Positive Control Oxford Immunotec
Quantiferon IGRA A positive IGRA (interferon gamma release assay) does not distinguish between latent and active TB – therefore need to investigate for active TB No false positives with BCG vaccination A negative IGRA does not rule out active TBand active/ latent TB in children – always need to inform and advise on the symptoms of TB
When to refer to the TB clinic If you suspect active TB Old untreated/treated TB and plans for anti TNF If IGRA positive If IGRA indeterminate or likely to be unreliable and plans for anti TNF
Latent TB infection • Screen and treat for latent TB infection in TB contacts under 65s • Screen and treatment for latent TB in patients from high incidence country in 16-35s • Screen for latent TB infection prior to biological therapy
Treatment for latent TB infection . • Counsel regarding lifetime risk of reactivation of 10% • Risk increased 5 fold by anti TNF • 2% risk of serious side effects • Orange urine and other secretions • Hepatotoxicity • Peripheral neuropathy • Interactions with other medication • Barrier contraception
Treatment . • Given prescription for full course of TB treatment • ( rifampicin and isoniazid for 3/12 or isoniazid for 6/12 • Meet TB nurses • Written and verbal information given • Arrange follow up • Contact details given
End of treatment . • Letter from patient and GP • Advised not to have repeat treatment for latent TB • Risk of new infection / reactivation is still possible • IGRA remains positive even after successful treatment
Conclusions • Refer contacts urgently if symptoms of TB • IGRA does not distinguish between latent and active TB • False negatives and indeterminate results can occur • Guidelines for screening of latent TB are confusing!