Download
1 / 30
330 likes | 1.3k Views
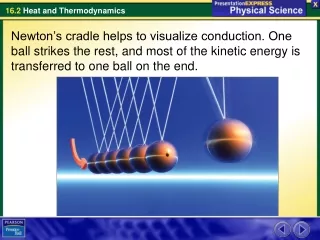
Ventricular Conduction Disturbances. Chapter 7. Bundle Branches. Normal conduction speed through the bundles is about 0.1 seconds. Bundle Branch Block. Consider a blocked or slowed branch or bundle. Right. Left. Right Bundle Branch Block. First Phase will be normal. Second Phase -

E N D
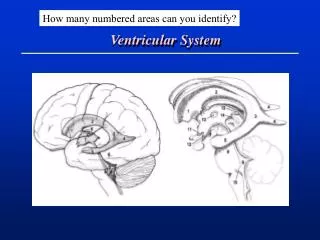
Ventricular Conduction Disturbances • Chapter 7
Bundle Branches • Normal conduction speed through the bundles is about 0.1 seconds
Bundle Branch Block • Consider a blocked or slowed branch or bundle Right Left
Right Bundle Branch Block First Phase will be normal Second Phase - Normal Third Phase - ? After the left ventricle has completely depolarized, the right ventricle continues to depolarize
Right Bundle Branch Block 1. 2. 3. 1. r wave in V1 q wave in V6 2. S wave in V1 R wave in V6 3. R’ wave in V1 S wave in V6
Right Bundle Branch Block Criteria • V1 or V2 = rSR’ - “M” or rabbit ear shape • V5 or V6 = qRS • Large R waves • Right chest leads: T wave inversion (“secondary changes” since they reflect a delay in depolarization not an actual change in depolarization). • Complete RBBB: QRS > 0.12 sec. • Incomplete RBBB: QRS = 0.10 to 0.12 sec.
Right Bundle Branch Block V1 = rSR’ V6 = qRS
Right Bundle Branch Block V2 = rSR’ V6 = qRS
Right Bundle Branch Block • Clinical Significance • Healthy heart • Organic heart disease • atrial septal defect • pulmonary disease • valvular lesions • degenerative changes in conduction system • chronic coronary artery disease • pulmonary embolism • after bypass graft surgery • Permanent or transient • RBBB by itself requires no treatment
Left Bundle Branch Block • RBBB affects mainly the terminal phase of depolarization • LBBB affects the early and terminal phases of depolarization • Septum is depolarized from right to left (rather than left to right) • Depolarization of the left ventricle takes longer
Left Bundle Branch Block 1. r wave in V1 R wave in V6 2. S wave in V1 R wave in V6
Left Bundle Branch Block • Loss of septal R in V1 and septal Q in V6. • Wide QRS • Negative in V1 • Positive in V6
Left Bundle Branch Block Criteria • Wide QRS complex • V1 = QS (or rS) and may have a “W” shape to it. • V6 = R or notched R showing a “M” shape or rabbit ears • Secondary T wave inversion • Secondary if in lead with tall R waves • Primary if in right precordial leads
RBBB versus LBBB ? ?
Left Bundle Branch Block • Causes • long standing hypertension • valvular lesion • cardiomyopathy • coronary artery disease • Precursor • Advanced CAD • Valvular heart disease • Hypertensive heart disease • Cardiomyopathy
Rate-Related (Exercise-Induced) Bundle Branch Blocks • Ischemia or other factors during exercise may produce BBB not seen at rest • Rate-limited bundle branch block • Exercise induced bundle branch block
Incomplete Bundle Branch Blocks • RBBB or LBBB where QRS is between .10 and .12 with same QRS features • Incomplete RBBB normal variant • Incomplete LBBB a progression of LVH
Intraventricular Delay or Intraventricular Conduction Defect General term for wide QRS complexes that are not typical of RBBB or LBBB
Tri-fascicular Conduction System • Right bundle • Left anterior (superior) fascicle • Left posterior (inferior) fascicle • Fascicular block (or hemiblock) = a block in either the LAF or LPF.
Fascicular Blocks • Fascicular blocks only slightly prolongs the QRS. • Fascicular blocks cause axis deviation as do infarcts and hypertrophy. • Left or right axis deviation without signs of infarct or hypertrophy are fascicular blocks.
Left Anterior Fascicular Block • Limb leads • QRS less width less than 0.12 sec. • QRS axis = Left axis deviation (-45° or more) • if S wave in aVF is greater than R wave in lead I • small Q wave in lead I, aVL, or V6
Left Posterior Fascicular Block • Right axis deviation (QRS axis +120° or more) • S wave in lead I and a Q wave in lead III (S1Q3) • Rare
Bifascicular Block • Two of the three fascicles are blocked. • Most common is RBBB with left anterior fascicular block.
Summary • The last component of the QRS vector will be shifted in the direction of the last part of the ventricles to be depolarized. • In other words, the major QRS vector shifts toward the regions of the heart that are most delayed in being stimulated. • RBBB: late QRS forces point toward the right ventricle (Rabbit ears, M shape in V1) • LBBB: late QRS forces point toward the left ventricle (negative in V1 and R or notched R in V6) • LAFB: late QRS forces point in a leftward and superior direction (LAD with deep S wave in aVF ).
Hypertrophy In The Presence of Bundle Branch Block • RVH and RBBB • RAD is typically seen; also look for RAE and its peaked P waves. • RBBB with RAD indicates RVH is likely present, too. • LVH and RBB • usual criteria can be used but also look for LAE