Download
1 / 82
990 likes | 1.9k Views
LTC Karen S. Vogt Pediatric Endocrinology, WRNMMCB March 2013. Rickets. PREP 2013 Content Specifications. Understand the necessity of adequate vitamin D intake in children and adolescents Understand the necessity of calcium and phosphorous intake in children and adolescents

E N D
LTC Karen S. Vogt Pediatric Endocrinology, WRNMMCB March 2013 Rickets
PREP 2013 Content Specifications • Understand the necessity of adequate vitamin D intake in children and adolescents • Understand the necessity of calcium and phosphorous intake in children and adolescents • Know that hypocalcemia with hypophosphatemia suggests vitamin D deficiency
PREP 2013 Content Specifications • Understand the mechanism of rickets in children with hepatic disease • Plan the treatment of a child with familial hypophosphatemic rickets
Outline • Case • Nutritional rickets and Vitamin D deficiecy • Prevention • Other types of rickets • PREP Questions
Case • 9 month old female presents in January for her well baby visit
History • Birth: • C-section at 34 weeks for placental abruption • Required PRBC transfusion x2 • PDA - closed after indomethacin x 1 • 18 day NICU stay • PMH: healthy • Immunizations: up-to-date
More History • Diet: exclusively breastfed until 6 months of age, now taking stage 2 baby foods and soft table foods • Meds: Poly-vi-sol in first 3 months of life, no current meds • Development: sits unsupported when placed, pulls to stand, cannot get from lying to sitting, immature pincer grasp, waves bye-bye, plays peek-a-boo, consonant babbling
History and Physical Exam • Family History: parents healthy, mom no longer taking prenatal vitamins, mom is Filipino, dad is half caucasian/half Filipino • Physical Exam : Unremarkable
Plan…. • Weight check in one month • Mom comes back in 2 weeks for concern for difficulty feeding • Less appetite for solids than previously and no weight gain from well visit
Labs • TSH, CRP, Celiac Panel – unremarkable • Fecal fat, reducing substances and alpha-1-antitrypsin – normal • Sweat test – normal • CMP- AlkPhos736 U/L (150-420) • Calcium 9.2 mg/dl (8.7-10.4) • Albumin 4.0 g/dl (3.5-5)
Labs • CBC - WBC 12.6 • Hgb10.8 • Hct34.7 • Plt 547 • MCV 64.6 (70-86)
Pediatric Endocrinology Consult • More History: Mom drinks no milk, occasional cheese, doesn’t like yogurt • Infant light skinned and born in early spring • Minimal time in the sun per mom – spent most of summer indoors • PE: subtle wrist widening, slight concavity of lateral chest walls, mild generalized low tone
More Labs…. • AlkPhos: 568 U/L (150-420) • Calcium: 8.8 mg/dl (8.7-10.4) • Albumin: 4.7 g/dl (3.5-5) • Corrected Ca: 8.24 mg/dl (8.7-10.4) • Phosphorus: 2.5 mg/dl (2.7-4.5) • PTH: 346.1 pg/ml (13-75) • 25 OH Vit D: < 4.0 ng/ml
Diagnosis • Rickets due to vitamin D deficiency • Treatment: • Ergocalciferol (Drisdol® 8000 IU/ml) 2000 IU daily • Calcium carbonate 40 mg/kg/day div bid
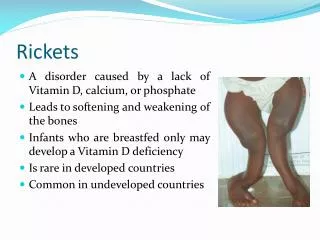
Rickets - Definition • Failure in the mineralization of newly synthesized bone matrix (osteoid) in growing bone • Due to deficiencies in calcium, phosphorous, or both • Most common cause is Vitamin D deficiency
Definitions • Osteomalacia – equivalent in mature bone • Contrast to osteoporosis • Low bone mass due to decreased mineralization and decreased bone matrix
Vitamin D - Sources • Dietary • Ergocalciferol (D2) – plant source • Cholecalciferol (D3) – animal source • UVB exposure • Promotes conversion of 7-dehydrocholesterol to cholecalciferol (D3) in the skin
Vitamin D Metabolism • Vitamin D is converted to 25(OH)D by 25-hydroxylase in the liver • 25(OH)D • A.k.acalcidiol • Inactive form • Reflects total body stores (2-3 week ½ life)
Vitamin D Metabolism • 25(OH)D is converted to 1,25(OH)2 D by 1α-hydroxylase in the kidney • 1,25-OH2 D • A.k.acalcitriol • Active form • More tightly regulated (4-6 hour ½ life)
1α-hydroxylase (kidney) • Stimulated by • PTH • Low phosphorous levels
1,25-OH2 Vitamin D • Acts on the vitamin D receptor (nuclear receptor) at the target organs • Major effect: absorption of calcium and phosphorous from the GI tract • Immunomodulary effects
Parathyroid Hormone (PTH) • Actions: keep serum calcium normal • Bone – stimulates reabsorption • Kidney: • Stimulates 1α-hydroxylase • Increases calcium reabsorption • Increases phosphate excretion • Stimulated by decreased serum calcium levels • Hypomagnesemia impairs its secretion
Alkaline Phosphatase • Produced by active osteoblasts, which form unmineralized matrix • Levels increase with increased osteoblast activity
Pathophysiology • Deficient GI absorption of : • Calcium → hypocalcemia → ↑PTH: • Release of calcium and phosphorous from bones • Activation of 1α-hydroxylase → increased formation of 1,25-OH2 D • Increase in renal phosphate loss • Phosphorous
Pathophysiology • Net effect: decreased calcium and phosphorous available for bone mineralization • Osteoid continues to form without mineralization • Expansion of the growth plate • Metaphyseal irregularities, fraying, flaring • Bones become “soft” and less rigid
Increasing Prevalence of Vitamin D Deficiency Rickets • Reasons for increasing prevalence • Exclusive breastfeeding • Breastfeeding moms with insufficient vitamin D stores • Increasing use of sunscreen • Less time spent outdoors Pediatrics 2008;122:398-417
Patient Risk Factors • Prematurity • Exclusive breastfeeing for 6 months (although was on poly-vi-sol for the first 3 months) • Probable vitamin D deficient breastfeeding mother • Winter season • Minimal sun exposure
Other Risk Factors – Vit D deficiency • Nutritional • Dark skin • Malabsorption • Obesity (sequestration in body fat) • Liver or kidney disease
Drugs • Anticonvulsants • Glucocorticoids • HIV medications • Rifampin • Isoniazide • Ketoconazole
Clinical Presentation - Rickets • Incidental finding • LE bowing • Delayed walking • Failure to thrive • Bone pain • Pathologic fracture • Hypocalcemia (to include seizure) • Weakness • Pneumonia, other respiratory infection • Anorexia • Restlessness/irritability
Physical Exam Findings • Poor growth or weight gain • Delayed anterior fontanelle closure • Teeth: delayed eruption, enamel defects • Generalized muscular weakness/hypotonia
Radiographic Findings • Wrist and/or knee films usually • Metaphyseal fraying, widening, flaring, cupping • Periosteum separated from the diaphysis • Generalized osteopenia
Associated Lab Findings • Iron deficiency anemia • Renal Fanconi syndrome
Vitamin D Deficiency Screening • Who? • Nonspecific symptoms: poor growth, gross motor delays, unusual irritability • Dark skin infants in higher latitudes in the winter and spring • Children taking chronic glucocorticoids or anticonvulsants • Chronic diseases associated with malabsorption • Frequent fractures and low BMD Pediatrics 2008;122:398-417
Vitamin D Deficiency Screening • How? • Serum Alkaline Phosphatase (ALP) • If elevated: 25 OH Vitamin D, PTH, Calcium and Phosphorus • Films: • Wrist • Knee Pediatrics 2008;122:398-417
Treatment of Vitamin D Insufficiency or Deficiency • < 1 month of age: 1000 IU/day • 1-12 months of age: 1000-5000 IU/ day • > 12 months of age: >5000 IU/day • Teens/adults: 50,ooo IU/week x 8 weeks • Consider Stoss therapy if compliance a concern (100,000 – 600,000 IU over 1-5 days) Pediatrics 2008;122:398-417
Vitamin D Preparations • Ergocalciferol = D2 (Drisdol®, Calciferol®) • Drops (8000 IU/mL) • Capsules (50,000 IU) • Injection (500,000 IU) – no longer available • Cholecalciferol = D3 • Capsules (5000 IU)