Download
1 / 52
1.07k likes | 4.34k Views
RICKETS. Presenter: Dr Suzanna Mwanza Moderator: Dr Pandey 02.10.13. HISTORY. CC, F/4 years, from Serenje First presented to UTH on 15 Feb 2013 Referred from Beit Cure hospital for management of Sickle Cell Disease (SCD)

E N D
RICKETS Presenter: Dr Suzanna Mwanza Moderator: Dr Pandey 02.10.13
HISTORY CC, F/4 years, from Serenje First presented to UTH on 15 Feb 2013 Referred from Beit Cure hospital for management of Sickle Cell Disease (SCD) Referral note said that patient was admitted at Beit Cure for orthopedic surgery for Right genuvalgum in SCD.
HISTORY PRESENTING COMPLAINTS • Inability to walk X 2 yrs HoPC • Started limping at 2 years of age • Mother says patient seemed weak • Gradual developed deformity of legs • Then eventually started failing to walk • Patient complained of pain in the legs • Slowly enlarging head since 3 years of age
HISTORY • No convulsion • History of jaundice • No history of pain passing urine or change in frequency of passing urine
HISTORY PAST MEDICAL HISTORY • Diagnosed with SCD at 2 yrs of age in Serenje • No history of stroke or trauma • No history of fractures • No history of Pnuemonia or recurrent respiratory infections • HIV neg
HISTORY DRUG HISTORY • On Folic acid • Did not take any vitamin supplements • Did not take any anticonvulsants or anti-acids ANTENATAL HISTORY • Mother spent time outdoors for significant part of a day • Had a varied diet that included local fish and eggs
HISTORY BIRTH HISTORY • Born at term at local clinic in Serenje, cried at birth, BWt- 2.7kg IMMUNISATION HISTORY • Fully immunised DEVELOPMENTAL HISTORY • Sat at 6 months • Crawled at – cannot remember • Stood at about 11 months • Walked at about 1 year 2 months
HISTORY NUTRITIONAL HISTORY • Breastfed exclusively till about 5 months of age till about 1 year and 6 months • Weaned on mealie meal porridge with groundnuts at 5 months • Did not receive formula milk • Started taking nshima with varied goods mainly vegetables – with local fish, eggs sometimes • Does not take cow milk • Ate 3 meals a day and one late afternoon snack • Following birth, was taken outside from about 4-6 weeks of age • Patient comes outside everyday and does not wear clothing that covers the whole body • Mother is a housewife and spends a significant part of her day outside
HISTORY FAMILY HISTORY • 2nd child in family of 2; first child died at birth following prolonged labour • No known history of SCD • No history of anyone with similar deformities, or of Rickets
EXAMINATION • Small for age, alert • P+, tinge of jaundice, Co, LNo • Afebrile • Oral cavity – dental caries • Ht – 86cm (below -3 SD) • Wt – 12.7kg (below -1 SD) • Wt/Ht – above median • HC – 55cm ( above +3 SD)
EXAMINATION Musculoskeletal: Head • Enlarged head - Caput quadratum • No craniotabes • No separated sutures and AF was closed • Bossing Chest • No rachitic rosary or harrison grooves Back • No spinal deformity – scoliosis or kyphosis Limbs • No widening of wrist and ankles • No anterior bowing of the tibia and femur • Able to stand unsupported, but walking with a limp with support • Genuvalgus of right knee and genuvarum of left knee (wind swept deformity)
EXAMINATION Cardiovascular: • tachycardia, haemic murmur Per abdomen: • Moderately distended, soft, non-tender, enlarged liver of 5cm, spleen not palpable Chest: • Vesicular breath sounds Central nervous system: • Neck supple, kernig’s negative • Normal tone in all limbs, power of 4 and normal reflexes
EXAMINATION • Urinalysis • Leukocytes – negative • Nitrites – negative • Urobilinogen – normal • Blood – negative • Bilirubin – negative • Protein – negative • Glucose – negative • Ketones - negative • pH – 6.0 • Specific gravity – 1.015
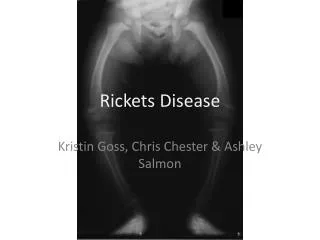
EXAMINATION Right genuvalgus and left genuvarus (windswept deformity) Anterior deviation of right knee
EXAMINATION No harrison grooves No rachitic rosary; protuberant abdomen
EXAMINATION Macrocephaly – HC 55cm (+3 SD) Bossing; caput quadratum
EXAMINATION Short stature Height – 86cm (-3 SD)
DIAGNOSIS • Rickets in • Sickle Cell Disease
INVESTIGATIONS • FBC, Diff • Urea, creatinine, Sodium, Potassium, LFTs • Calcium, Phosphate, ALP, PTH, 25 Vit D, 1,25 Vit D • High performance liquid chromatography (HPLC) • X-ray of skull and upper and lower limbs • Folic acid • Deltaprim • Vitamin D3 – 5000U/day
X-rays X-ray of lower limbs – AP view Reduced bone density (rarefication) Widening of distal ends of femur and proximal and proximal end of tibia X-ray of ankle joints – AP view Cupping of distal end of tibia
X - rays Right ankle joint – lateral view Splaying of metaphyseal end of bone Widening of distal end of metaphysis Fraying of metaphysis Left ankle joint - lateral view Reduced bone density
X- rays Wrist joints – lateral view Mild widening of the distal radius Wrist joints – AP view Mild widening of distal radius
X-rays Skull X-ray – AP view No hair-on-end appearance Skull X-ray – lateral view No hair-on-end appearance
Follow up • Started on Vit D 400IU on day 11 post-adm (2 tablets daily of Osteocare – the only available source of Vit D at UTH at the time) • Discharged on day 11 for review after 1 month • Folic acid, Deltaprim, Vit D
Review – one month later • Mother had purchase Vit D and was giving 1000U/day • Mother had noted improvement • Patient was walking without support • Changed to Vit D 5000U/day for 6 months • Orthopaedic surgical correction of limbs if there was no improvement in 6 months • Review in 6 months
Final diagnosis DIAGNOSIS • Vitamin D deficiency (nutritional) Rickets • High phytate diet (high fiber diet) • ? Low calcium diet • Sickle Cell Anaemia
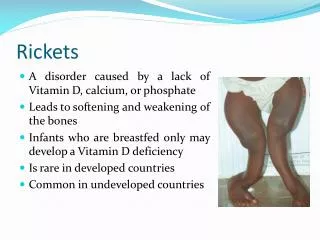
REVIEW OF RICKETS • Rickets is a disease of growing bones which occurs in children only before the fusion of epiphyses and is due to unmineralised matrix at the growth plates • Osteomalacia is due to inadequate mineralization of bone osteoid and occurs in children and adults
Risk factors for nutritional Rickets • Exclusive breastfeeding • (insufficient Vit D concentrations 20-60 IU/L as opposed to 200 IU/L recommended in infants) • Maternal vitamin D deficiency • Living in temperate climates • Lack of sunlight exposure • Darkly pigmented skin • Social and religious customs that prevent sunlight exposure • Low dietary calcium intake • High phytate content in diet (unrefined cereal; impairs intestinal calcium absorption)
Phytate in diet • Grains and leafy vegetables are high in phytateand oxalate which decrease intestinal absorption of dietary calcium • In rats, high phytate diet results in increased catabolism of 25-Vit D to inactive metabolites and increased excretion of these products in stool resulting in reduction of 25-Vit D concentration • In humans, half life of 25-Vit D reduced to nearly 40% among patients on high fiber diets • Studies in South Africa, Nigeria, Bangaladesh and UK Asians show that rickets was due to low calcium diet and high phytate diets (unrefined cereals) • Mean age of presentation around 4 year in calcium deficiency rickets; adolescence for vit D deficiency rickets Pettifor JM, 2004, Nutritional rickets: deficiency of vitamin D, calcium or both?, Am J ClinNutr; 80 (suppl):1725S-9S
VITAMIN D DISORDERS Nutritional Vitamin D deficiency Congenital Vitamin D deficiency Secondary Vitamin D deficiency Malabsorption Increased degradation Decreased Liver 25-hydroxylase Vitamin D dependent ricket Type 1 Vitamin D dependent ricket Type 2 Chronic Renal Failure PHOSPHORUS DEFICIENCY Inadequate intake Premature infants Aluminium containing antacids CALCIUM DEFICIENCY Low intake Diet Premature Infant Malabsorption Primary Disease Dietary inhibitors of calcium absorption RENAL LOSSES X- linked hypophosphatemicricket AD hypophosphatemicricket Hereditary hypophosphatemicricket with hypercalcuria Overproduction of phosphatonin Tumors induced rickets Mccunealbright syndrome Epidermal nevus syndrome Neurofibromatosis Fanconi syndrome Dent Disease Causes of Rickets
Phosphatonin • Phosphatonin is a humoral mediator that decreases renal tubular reabsorption of phosphate and thus decreases serum phosphorus • Also decreases activity of renal 1 alpha hydroxylase causing decreased production of 1,25 Vit D • Fibroblast growth factor-23 (FGF-23) is the most well characterised phosphatonin • Increased levels of phosphatonin cause many of the phosphate-wasting diseases
Clinical features GENERAL •Failure To Thrive •Listlessness •Protruding Abdomen •Muscle Weakness (specially proximal) •Fractures HYPOCALCAEMIC SYMPTOMS •Tetany •Seizures •Stidor due larngeal spasm HEAD •Craniotabes •Frontal Bossing •Delayed Fontanelle Closure •Delayed Dentition •Craniosynostosis
Clinical features CHEST • Rachitic rosary • Harrison Groove • Pectuscarinatum • Thoracic asymmetry • Widening of thoracic bone • Respiratory Infections • Atelectasisimpairment of air movement
Clinical features BACK • Scoliosis • Kyphosis • Lordosis EXTREMITIES • Enlargement of wrist or ankle • Valgus and varus deformities
INVESTIGATIONS Edge of metaphysis loses its sharp border FRAYING Edge of metaphysis changes from convex or flat surface to a more concave surface CUPPING (most easily seen at distal ends of radius, ulna and fibula) Widening of Metaphyseal end of bone SPLAYING Metaphyseal lines spread laterally forming CORTICAL SPURS Widening of distal ends of metaphysis (A-Normal, B-Rickets)
Other Radiological Findings • Changes of diaphysis – appear a few weeks later • Coarse trabeculation • generalized rarefaction • Cortical thinning • Subperiosteal erosion