Download
1 / 58
580 likes | 648 Views
Explore the causes, symptoms, and implications of rickets, a bone disease linked to vitamin D deficiency. Learn about its pathogenesis, epidemiology, and physiological effects on bone health.

E N D
Rickets and Tetania CONF. DR. INGRITH MIRON DR. ADRIANA MOCANU
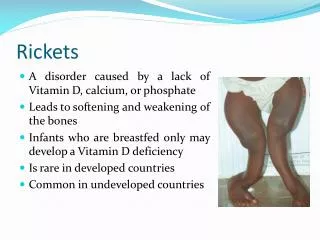
DEFINITION • Disease of growing bones in which defective mineralisation occurs in both bone and cartilage of epiphyseal growth plate, associated with: • Growth retardation • Skeletal deformities
Epidemiology • Vitamin D deficiency in pediatric patients has seriousimplications for both childhood well-being as well aslifelonghealth. • Vitamin D is well known for its role as a mediator ofcalcium homeostasis, and in the development and maintenance of theskeleton • Alarming prevalence of medical problems related to thisnutritional problem, ranging from severe nutritional ricketsto subclinical vitamin D deficiency, even withinindustrializedsocieties
Sources of Vitamin D • Sun light • Synthesis in the body from precursor sterol • All Milk products (fortified) • Fish liver oil • Egg yolk
Physiology of vitamin D Cholecalciferol (ie, vitamin D-3) - formed in the skin from 5-dihydrotachysterol. hydroxylation in 2 steps: - first hydroxylation : position 25 (liver) →calcidiol (25-hydroxycholecalciferol):good indicator of overall vitamin D status; - second hydroxylation: 1 position (kidney) →active metabolite calcitriol (1,25-dihydroxycholecalciferol).
Physiology of vitamin D • Calcitriol promotes: • absorption of calcium and phosphorus from the intestine, • increases reabsorption of phosphate in the kidney, • acts on bone to release calcium and phosphate, • directly facilitate calcification
Physiology of vitamin D These actions increase the concentrations of calcium and phosphorus in extracellular fluid : • leads to the calcification of osteoid, primarily at the metaphyseal growing ends of bones but also throughout all osteoid in the skeleton; • Parathyroid hormone facilitates the 1-hydroxylation step in vitamin D metabolism.
Pathogeny • The primary pathology : defective mineralisation of bone matrix • The primary bone matrix mineral = hydroxyapatite = Ca10(Po4)6(OH)2 • Any disease that limit the availability of calcium or phosphate will lead to rickets • 2 main categories • Hypocalcaemia rickets • Disfunctions of vitamin D metabolism or vitamin D action • Hypophosphatemic rickets • Abnormalities of phosphate metabolism
Pathogeny In the vitamin D deficiency : hypocalcemia: • stimulates excess parathyroid hormone→ stimulates renal phosphorus loss→ reducing deposition of calcium in the bone; • Excess parathyroid hormone : produces changes in the bone similar to those occurring in hyperparathyroidism. • Early in the course of rickets, the calcium concentration in the serum decreases; • parathyroid response, the calcium concentration usually returns to the reference range, though phosphorus levels remain low; • Alkaline phosphatase (produced by overactive osteoblast cells) leaks to the extracellular fluids so that its concentration rises to anywhere from moderate elevation to very high levels.
Pathogeny The main anomalies of phosphocalcic balance resulting in : • intestinal malabsorption of calcium and phosphorus due to deficiency of vitamin D and secondary hyperparathyroidism. • the sequence of main steps in vitamin D deficiency causes a tendency to hypocalcemia with changing ratio Ca / P and the occurrence of compensatory secondary hyperparathyroidism (PTH ↑) produces calcium mobilization from bone and renal phosphorus removal - what makes the SEC ions to be inadequate mineralization, leading to: • ossified matrix; • calcifying osteoid tissue; • deformed bone static and mechanical; • deformities typical of rickets.
ETIOLOGY • Nutritional: commonest cause in the developing countries • Malabsorption • Drugs that increases metabolism of vitamin D in the liver • Chronic liver disease • Renal rickets • Chronic renal failure • Hereditary rickets • Vitamin D dependent rickets ( Type 1& 2) • Vitamin D resistant rickets
Nutritional Causes Lack of vitamin D • Commonest cause in Saudi Arabia and in developing countries • Lack of exposure to U/ V sun light • Dark skin • Covered body • Kept in-door • Exclusive breast feeding • Limited intake of vitamin –D fortified milk and diary products • During rapid growth • Infancy • puberty
Except in pediatric patients with chronic malabsorption syndromesor end-stage renal disease, nearly all cases of rickets occur in breastfed infants who have dark skin and receive no vitamin D supplementation. Incidence in Europe is similar to that in the United States. In sunny areas, such as in the Middle East, rickets may occur when infants are bundled in clothing and are not exposed to sunlight.
Clinical features • The earliest sign of rickets in infant is craniotabes (abnormal softness of skull) • Delayed closure of anterior fontanel • Widening of the forearm at the wrist (widened metaphysis= area between epiphysis and diaphysis) • Rachitic rosary • Swelling of the costo-chondral junction • Harrison’s groove • Lateral indentation of the chest wall at the site of attachment of diaphragm • Bowing of tibia and fibula may be observed at any age • Growth retardation due to impaired calcification of bone epiphysis (epiphysis= area of growth plates) • Hypocalcaemic manifestations • hypotonia • Seizure, tetany,muscle weakness, paraesthesia, numbness
Biochemical findings of rickets Vitamin D deficiency rickets • Low- normal serum calcium level • Increased secretion of PTH (secondary hyperparathyroidism) to compensate for low calcium • Hyperparathyroidism will increase renal excretion of phosphate, leads to low serum phosphate level • Elevated alkaline phosphatase enzyme • Reduced urinary calcium level • Low level of both 25 and 1,25- dihydroxy vitamin D • Elevated parathyroid hormone level
Rickets Biochemical findings
Rickets Biochemical finding
Radiological findings of rickets • Generalized osteopenia • Widening of the unmineralised epiphyseal growth plates • Fraying of metaphysis of long bones • Bowing of legs • Pseudo-fractures (also called loozer zone) • Transverse radio lucent band, usually perpendicular to bone surface • Complete fractures • Features of long standing secondary hyperparathyroidism (Osteitis fibrosa cystica) • Sub-periosteal resorption of phalanges • Presence of bony cyst (brown Tumor)
Rikcets - diagnosis • History & physical examination finding • Radiographic abnormality • Special etiology confirmed with biochemical tests
Rickets:Differential diagnosis 1.Hereditary Rickets: • Hypophosphatemic rickets (Vit D resistant) • Vitamin D dependent rickets
Rickets:Differential diagnosisHypophosphatemic Rickets • X-linked dominant / Autosomal dominant • Males affected more than females • Commonest inherited form of rickets • Prevalence 1: 25000 • Phosphate wasting by renal tubules leads to: • Low serum phosphate • Normal calcium • In-appropriate low or normal 1,25-di hydroxy vitamin D • phosphate is the major stimulus for 1 hydroxylase • Severe rickets and short stature by 1-2 years
Rickets:Differential diagnosisHypophosphatemic Rickets • Nutritional phosphate deficiency • Prematurity • Decreased intestinal absorption of phosphate • Ingestion of phosphate binders (aluminum hydroxide) • Renal phosphate wasting • RTA • Vitamin D resistant rickets • Tumor induced osteomalacia (oncogenicosteomalacia)
Rickets:Differential diagnosisHypophosphatemic Rickets Biochemical findings : • Low serum phosphate level • Normal calcium level • Normal parathyroid hormone level • High alkaline phosphatase level • In-appropriate low or normal 1,25-di hydroxy vitamin D • phosphate is the major stimulus for 1 hydroxylase
Rickets:Differential diagnosisVitamin D dependent rickets Type 1 • Rare, autosomal recessive • Lack of 1 hydroxylase enzyme • Clinically and Biochemically similar to nutritional rickets except it appears early at 3-4 months Type 2 • Rare autosomal recessive disorder • 1 hydroxylase enzyme is present • Lack of Calcitriol receptors • Common in Arabs • Baldness • Severely affected individuals • Unresponsive to treatment
Rickets:Differential diagnosis 2)Celiac disease 3)Pancreatic insufficiency • Cystic fibrosis 4)Hepato-biliary disease • Biliary Atresia • Cirrhosis • Neonatal hepatitis 5)Drugs • Anti-convulsants • Phenobartbital • Phenytoin 6)Diet • Excess of phytate in diet with impaired calcium absorption (cereals, flour)
Rickets:Differential diagnosis Chronic liver disease • Cirrhosis reduces 25-hydroxylation of vitamin D • Biliary obstruction: • prevents absorption of fat soluble vit D • Interrupts its enterohepatic circulation
Rickets:Differential diagnosis Chronic renal failure • Reduces 1 hydroxylation of 25 hydroxy vitamin D leads to low concentration of 1,25-di hydroxy vitamin D • Consequently impair calcium absorption from the gut • Renal osteodystrophy • Osteitisfibrosacystica due to long standing secondary hyperparathyroidism When GFR falls below 30 ml/min/1.73m2 • Impaired growth • Osteitisfibrosa results • Sub-periostealresorption at middle and distal phalanges • Bone pain • Muscle weakness
Rickets:Differential diagnosis Renal Tubular Acidosis (RTA) • Metabolic acidosis from proximal or distal tubular disease • Renal wasting of calcium (hypercalciuria) • Accompanied with other urinary loss: • Phosphate • Glucose • Protein • Isolated or generalized forms • Fanconi (generalized form of RTA) • Associated with cystinosis, tyrosinemia, Wilson's disease
Treatment • Treatment may be gradually administered over several months or in a single-day dose of 15,000 mcg (600,000 U) of vitamin D • gradual method 125-250 mcg (5000-10,000 U) daily for 2-3 months until healing is well established and the alkaline phosphatasenormal Intramuscular injection is also available 200 000 ui X 3 doseseveryotherday • In nutritional rickets, the phosphorous level rises in 96 hours and radiographic healing is visible in 6-7 days
Treatment From birth to 18 months • The recommended dose to the newborn to 18-month 500 IU / day. • Increasing the dose of 1000 - 1500 IU / day for a limited period of time is required in some cases to: • small infants whose mothers did not receive vitamin D prophylaxis during pregnancy; • dismaturii premature and at least the first month of life. • young infants (up to 3-4 months) born in cold weather. • infants with frequent acute illnesses and those with frequent and prolonged hospitalizations. • children in polluted environments. • Children with skin hyperpigmentation.
Treatment • children with poor environmental conditions. • children in some residential institutions (swing, orphanages) that move less air and less out in the sun. • Children with chronic anticonvulsant therapy (phenytoin, phenobarbital), cortisone In such situations will be given vitamin D daily dose of 1500 IU / day, but not more than one month, and then restarted at 400-500 IU or 500 IU alternate dose 1-2 weeks at a dose of 1000 IU; generally higher doses of 1500 IU are therapeutic
Treatment After 18 months • Vitamin D is administered only during the months of the year neînsorite with R, from September to the end of April until the age of 12-15 years. • dose: daily 400-500 IU or every 7-10 days by 4000-5000 IU Vitamin D is given in oil solution (Vit. A + D2) administered po • only fractional administration of vitamin D is physiological, as it ensures a good, especially if vitamin D is given a meal of milk;
Treatment • If severe deformities have occurred, orthopedic correction may be required after healing. Most of the deformities correct with growth. • Human milk contains little vitamin D and contains too little phosphorus for babies who weigh less than 1500 g. • Infants less than 1500 g need supplementation (ie, vitamin D, calcium, phosphorus) if breast milk is their primary dietary source.
Treatment Curative treatment of rickets Objectives: • prevention or correction of skeletal deformities of rickets and secondary hyperparathyroidism reagent; • prevention and correction hiopocalcemiei and related symptoms (tetany, sudden death); • ensure normal growth and development; • application of vitamin D dose to provide a therapeutic effect while avoiding adverse effects that: hypercalcemia, hypercalcuria.
Treatment Lifestyle and nutrition • It is important in the treatment and prevention of rickets triggered the disease. Preventive measures add the following recommendations: • - Child with rickets evolving not be encouraged early to sit nor stand up and walk to the stabilization of the disease. • - Recommend wearing supportive shoes with soles or you can, bare foot up to age 3.
Treatment Curative therapy (schemes): Mild and medium forms: - oral daily administration - 2000-4000 IU Vitamin D for 6-8 weeks and then returned to prophylactic - typically for 6 months each 1000 IU / day). Severe forms: manifest hypocalcemia (convulsions) and children with malabsorption. - administration of 3 doses of 100 000 UI Stoß vitamin D2 or D3 intramuscularly every 3 days, then a dose of 200 000 IU after 30 days oral or i.m.
Rickets:Evolution and prognosis Evolution is generally favorable when rickets is controlled. Evolution untreated rickets-consequences: 1. Immediate consequences: - recurrent respiratory infections (favored by excessive flexibility and muscular hypotonia chest -lung rickety); - poor psychomotor development - hypocalcemia in infants caused certain complications: tetanie, laryngospasm, convulsions; - development of a microcytic,hypochromic anemia 2. Late consequences : - bone changes in the knees (genuvarum, genuvalgum) ; -signs of bone may persist for some time after correcting biological syndrome florid rickets, and in this case they do not require the setting treatment.
Rickets:Evolution and prognosis Evolution of treated rickets : - Clinical signs within 2-4 weeks; • Biochemical normalization in 2-4 weeks, • in 1-5 days hypocalcemia, • hypophosphatemia and hyperparathyroidism in 2-3 weeks. • alkaline phosphatase activity levels remain elevated for several weeks (6-8 weeks), to complete the correction of the deficiency bone mineralization, is a biological marker of cure of rickets. • 25 OHD plasma levels to normal within 1-2 days. - Improving radiological observed 2-4 weeks after beginning treatment with vitamin D in the form of dense linear deposits in the metaphyseal lines. Epiphyses and metaphyses is found normalization after 3 months.
TETANIA (Hypocalcemia) Definition Spasmophilia or tetanys -pathological states of the central nervous system and peripheralnervous system due to extracellular ionic changes involved in the function of neurons and peripheral nerves.
A 70-kg person has approximately 1.2 kg of calcium in the body, stored as hydroxyapatite in bones (>99%). 1% (5-6 g) of this calcium is located in the intracellular and extracellular compartments, with only 1.3 g located extracellularly. calcium concentration in the plasma is 4.5-5.1 mEq/L (9-10.2 mg/dL) fifty percent of plasma calcium is ionized, 40% is bound to proteins (90% of which binds to albumin
Pathophysiology • Ionized calcium is the necessary plasma fraction for normal physiologic processes. In the neuromuscular system, ionized calcium levels facilitate nerve conduction, muscle contraction, and muscle relaxation • Normocalcemia requires PTH and normal target-organ response to PTH • PTH stimulatesosteoclastic bone reabsorptionanddistal tubular calciumreabsorptionandmediates 1,25-dihydroxyvitamin D (1,25[OH]2 D) intestinal calciumabsorption.
Pathophysiology • Vitamin D stimulates intestinal absorption of calcium, regulates PTH release by the chief cells, and mediates PTH-stimulated bone reabsorption • A reduction in total serumcalciumcanresultfrom a decrease in albuminsecondarytoliverdisease, nephroticsyndrome, or malnutrition. • Hypocalcemiacauses neuromuscular irritabilityandtetany. • Alkalemiainducestetanydueto a decrease in ionizedcalcium, whereasacidemiais protective.
Tetania Clinical classification distinguishes two forms: 1. tetany manifested - manifested by seizures (CNS excitability), carpopedal spasm (peripheral motor nerves) and paresthesias (sensory nerves). 2. latent tetany or spasmophilia - characterized by motor expressions obtained by a trigger such as ischemia, hyperpnea, electrical or mechanical stimulation.
Tetania- etiological classification I. Hypocalcemictetany The need for calcium: 50mg/kg/zi. Contributing factors are artificial alimentation, season without sun, prematurity, neonatal infection, meso-diencephalic impairments, nephropathy. a) parathyroid hypocalcemictetany: 1. Transient hypoparathyroidism of newborn (high birth weight, diabetic mothers, hypoxia); 2. Primary congenital hypoparathyroidism - rare; 3. Secondary hypoparathyroidism; 4. Pseudo-and pseudo-pseudohipoparatiroidismul characterized by resistance to parathyroid hormone target organs.
Tetania- etiological classification I. Hypocalcemic tetany b) hypocalcemic tetany deficiency of vitamin D or vitamin D metabolic abnormalities: - deficiency rickets ; - steatorrhea secondary rickets; - vitamin D resistant rickets. Hypocalcemia may occur at certain stages of rickets (I and III).
Tetania- etiological classification II. Hypomagnesiemictetany - low magnesium and calcium; - Hypocalcemia is due to reduced release of endogenous PTH, alteration organ response to PTH and possible alteration of gastrointestinal absorption of calcium. III. Tetany with normal calcium - normal serum calcium, decreases calcium ion fraction or psychogenic tetany of adolescent with normal calcium
Tetania- etiological classification IV. Other causes: - Alkalosis; - Hypernatremia plus potassium deficiency (Conn's syndrome) due to primary aldosteronism; - Postacidotic (in severe diarrhea); - Chronic renal failure; • Blood transfusions citrate in large quantities. • Critical illness and severe sepsis • Aftercorrection of thyrotoxicosis • Acute pancreatitis • Drugs: Bisphosphonates, Anticonvulsanttherapy , Foscarnet, Ethylenediaminetetraacetic acid (EDTA) , Fluoridepoisoning
Tetania – clinical manifestations • numbness and tingling sensations in the perioral area or in the fingers and toes • muscle cramps, particularly in the back and lower extremities; may progress to carpopedal spasm (ie, tetany) • wheezing; may develop from bronchospasm • abdominal pain, • dysphagia • voice changes (due to laryngospasm)
Tetania – clinical manifestations • irritability, impairedintellectualcapacity, depression, andpersonalitychanges • fatigue • seizures(eg, grand mal, petit mal, focal) • otheruncontrolledmovements • chesttightness, • ticks, twitch, headache, dizziness, confusionalepisodes, • insomnia or restlesssleep, sweating, • cardiovascular signs:tachycardia, hypertension or breathing - shallowtachypnea.
Tetania – clinical manifestations Maneuvers to to induce neuromuscular hyperexcitability: a) ischemia - Trousseau sign. The cuff pressure is applied for 3 minutes at a medium pressure and motor follows the occurrence of events. b) mechanical stimulation (percussion) of the peripheral nerves - Facial nerve - Chvostek sign; - Peroneal nerve - Lust sign (dorsiflexion and abduction of the foot); - Orbital apophysis - mark Weiss (upper eyelid orbicularis). c) electrical stimulation – Erb sign: response to electrical stimulation of the motor nerves galvanic current, of lower intensity than physiological.