Download
1 / 35
551 likes | 1.06k Views
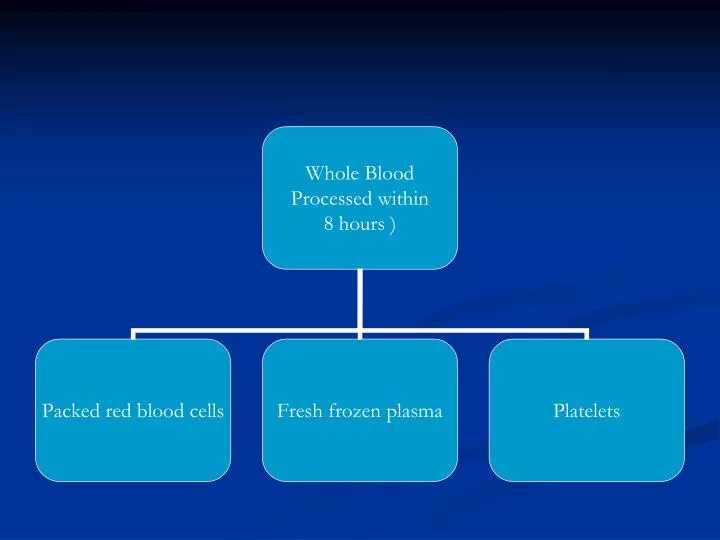
Plasma + Platelets. Whole blood. Buffy. RBC. Component preparation. Principle - Differential centrifugation Red cells Packed cells Red cells + additive Plasma Bank plasma Fresh frozen Cryo supernate Platelets Platelet rich concentrate Platelet rich plasma Cryoprecipitate.

E N D
Plasma + Platelets Whole blood Buffy RBC Component preparation • Principle - Differential centrifugation • Red cells • Packed cells • Red cells + additive • Plasma • Bank plasma • Fresh frozen • Cryo supernate • Platelets • Platelet rich concentrate • Platelet rich plasma • Cryoprecipitate
DEFINITIONS BLOOD PRODUCT = Any therapeutic substance prepared from human blood WHOLE BLOOD = Unseparated blood collected into an approved container containing an anticoagulant preservative solution BLOOD COMPONENT = 1. A constituent of blood , separated from whole blood such as • Red cell concentrate • Plasma • Platelet concentrates 2. Plasma or platelets collected by apheresis 3. Cryoprecipitate prepared from fresh frozen plasma
Blood Components THE PRBC Storage - 2 – 6 O C Unit of issue - 1 donation ( unit or pack ) Administration - ABO & Rh compatible - Never add medication to a unit - Complete transfusion within 4 hrs of commencement Member 1
Dosage & Administration Dosage - 1 unit/10 kg body wt Adult dose is 4-8 units Administration - Preferably ABO & Rh group specific but not essential Other groups can be used
PLATELETS • Platelet units can be either • Random donor units • Apheresis units • 1 random donor unit contains 55 x109 platelets • 1 apheresis unit contains 240x109
Guidelines for Platelet Tx. Mild - 50,000-1,00,000/µl Tx - usually not required Moderate - 20,000-50,000/µl Tx-if symptomatic or has to undergo surgery/trauma Severe - < 20,000/µl Risk of bleeding - high Prophylactic Tx
Indications for platelet transfusion BLEEDING due to thrombocytopaenia Due to platelet dysfunction Prevention of spontaneous bleeding with counts < 20,000
IMPORTANT PRECAUTIONS Stored at 20-24 Degree celcius. Constantly agitated Only last for 5 days Infused in 30 mins
Fresh Frozen plasma • Fresh frozen plasma – labile & nonlabile clotting factors, albumin and immunoglobulin. Factor VIII ( 8 ) level at least 70 % of normal fresh plasma level Storage - 20 C for 1 yr, - 65 C for 7 yrs. • Before use thawed at 37 o C
Fresh frozen plasma Indications - Replacement of multiple coagulation factor deficiencies eg • Liver disease • Anticoagulant overdose • Depletion of coagulation factors in pts receiving large volume transfusions • DIC (disseminated intravascular coagulation)
FRESHFROZEN PLASMA Indication • Clinically significant deficiency of Factors II, V, X, XI • Replacement of multiple coagulation factor deficiencies :- liver disease , warfarin treatment, dilutional and consumption coagulopathy Contraindication • Volume expansion • Immunoglobulin replacement • Nutritional support • Wound healing
FRESH FROZEN PLASMA MD-3-49 Precaution • Acute allergic reaction are common • Anaphylactic reaction may occur • Hypovolemia alone is not an indication for use Dosage - Initial dose of 15 - 20 ml / kg Administration • Must be ABO compatible, Rh not required • Infuse as soon as possible after thawing ( within 6 hrs ) • using standard blood administration set
FFP Fresh Frozen Plasma Plasma collected from single donor units or by apheresis Frozen within 8 hours of collection -40o C Can last for a year
Dosage & Administration for FFP Dosage - 10-15 ml/Kg(Approx 2-3 bags for an adult) Administration - Thawed at +37o C before transfusion ABO compatible Group AB plasma can be used for all patient
Risk Benefit Analysis risk > benefit benefit > risk Hb gm/dl 4 5 6 7 8 9 10 11 12 13 14 why transfuse why not transfuse individual patient factors decide transfusion trigger
Time Limits for Infusion Blood/ Start infusion Complete infusion blood product Whole blood/ within 30 min. of within 4 hour red cells removing pack (less in high from ambient temperature) refrigerator Platelet immediately within 20 min concentrates FFP within 30 min within 20 min
TRANSFUSION REACTIONS @RBC’s ! • Nonhemolytic 1-5 % transfusions Causes -Physical or chemical destruction of blood: freezing, heating, hemolytic drug -solution added to blood -Bacterial contamination : fever, chills, urticaria • Slow transfusion, diphenhydramine , antipyretic for fever • Hemolytic • Immediate: ABO incompatibility (1/ 12-33,000) with fatality (1/ 500-800,000) Majority are group O patients receiving type A, B or AB blood Complement activation, RBC lysis, free Hb (+ direct Coombs Ab test)
Chills , fever Facial flushing Hypotension Renal failure DIC Chest pain Dyspnea Generalized bleeding Hemoglobinemia Hemoglobinuria Shock Nausea Vomitting Back pain Pain along infusion vein Signs and Symptoms of AHTR
Anesthesia: hypotension, urticaria, abnormal bleeding • Stop infusion, blood and urine to blood bank, coagulation screen (urine/plasma Hb, haptoglobin) • Fluid therapy and osmotic diuresis • Alkalinization of urine (increase solubility of Hb degradation products) • Correct bleeding, Rx. DIC
@WBC’s! • Europe: All products leukodepleted • USA: Initial FDA recommendation now reversed pending objective data (NOT length of stay for expense) • Febrile reactions • Recipient Ab reacts with donor Ag, stimulates pyrogens (1-2 % transfusions) • 20 - 30% of platelet transfusions • Slow transfusion, antipyretic, meperidine for shivering
TRALI (Transfusion related acute lung injury) • Donor Ab reacts with recipient Ag (1/ 10,000) • noncardiogenic pulmonary edema • Supportive therapy
Transfusion-related Acute Lung Injury (TRALI) Acute and severe type of transfusion reaction Symptoms and signs • Fever • Hypotension • Tachypnea • Dyspnea • Diffuse pulmonary infiltration on X-rays • Clinical of noncardiogenic pumonary edema
Transfusion-related Acute Lung Injury(TRALI) Therapy and Prevention • Adequate respiratory and hemodynamic supportive treatment • If TRALI is caused by pt. Ab use LPB • If TRALI is caused by donor Ab no special blood components
Transfusion-associated Graft-versus-HostDisease ( TA-GVHD) • Rare: immunocompromised patients • Suggestion that more common with designated donors • BMT, LBW neonates, Hodgkin's disease, exchange Tx in neonates
Graft-versus-Host Reaction Signs & Symptoms • Onset ~ 3 to 30 days after transfusion • Clinical significant – pancytopenia • Other effects include fever, liver enzyme, copious watery diarrhea, erythematous skin erythroderma and desquamation
@Platelets! Alloimmunization • 50 % of repeated platelet transfusions • Ab-dependent elimination of platelets with lack of response • Use single donor apheresis • Signs & Symptoms • mild slight fever and Hb • severe platelet refractoriness with bleeding Post-transfusion purpura • Recipient Ab leads to sudden destruction of platelets 1-2 weeks after transfusion (sudden onset) • Rare complication
INFECTIOUS COMPLICATIONS I. Viral (Hepatitis 88% of per unit viral risk) Hepatitis B • Risk 1/ 200,000 due to HBsAg, antiHBc screening (7-17 % of PTH) • Per unit risk 1/63-66,000 • 0.002% residual HBV remains in ‘negative’ donors (window 2-16 weeks) • Anti-HBc testing retained as surrogate marker for HIV
NANB and Hepatitis C • Risk now 1/ 103,000 (NEJM 96) with 2nd/ 1/ 125,000 with 3rd generation HCV Ab/ HVC RNA tests • Window 4 weeks • 70 % patients become chronic carriers, 10-20 % develop cirrhosis
HIV • Current risk 1/ 450- 660,000 (95) • With current screening (Abs to HIV I, II and p24 Ag), window 6-8 weeks (third generation ELISA tests in Europe) • sero -ve window to < 16 days
HTLV I, II • Only in cellular components (not FFP, cryo) • Risk 1/ 641,000 (window period unknown) • Screening for antibody I may not pick up II CJD (and variant CJD)
II. Bacterial • Contamination unlikely in products stored for > 72 hours at 1-6 0 C • gram –ve, gram +ve bacteria most frequent – Yersinia enterocolitica Produced endotoxin Platelets stored at room temperature for 5 days, with infection rate of 0.25% III. Protozoal • Trypanosoma cruzi (Chaga’s disease) • Malaria • Toxoplasmosis • Leishmaniasis
Serological Testingfor Infectious markers • HIV – Ag • Anti – HIV • HBsAg • Anti – HCV • Test for syphilis
METABOLIC COMPLICATIONS Citrate toxicity • Citrate (3G/ unit WB) binds Ca2+ /Mg+ • Metabolized liver, mobilization bone stores • Hypocalcemia ONLY if > 1 unit/ 5 min or hepatic dysfunction • Hypotension more likely due to cardiac output/ perfusion than calcium (except neonates) • Worse with hypothermia/ hepatic dysfunction