Download
1 / 60
640 likes | 998 Views
Learn about the goals and methods of donor screening, including medical history questionnaires, physical examinations, and informed consent procedures to ensure the safety of blood donations and prevent disease transmission.

E N D
Goals of Donor Screening • Screen for diseases/conditions for which there are no tests • Reduce demand for detection of infectious agents by tests • Reduce window period collections • Prevent collection of infectious units
Donor Screening Donor screening encompasses the donor medical history, mini physical examination, and serologic testing of the donor blood. • Donor identification and registration requirements to confirm donor identity and link the donor to existing donor records • Consent to donate • Additional information
Donor Screening • Reasons for donor screening • Ensures safety of the donation for the donor • Obtains donor blood with a reduced risk of transmitting disease to the potential recipient
Medical History Questionnaire • A standardized medical history questionnaire • Self-administered questionnaires must be reviewed by trained personnel prior to blood collection.
Donor History Questionnaire (DHQ) • The currently approved version of the Donor History Questionnaire (DHQ) can be downloaded from the FDA website. http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/LicensedProductsBLAs/BloodDonorScreening/UCM213552.pdf
DHQ Flowcharts • http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/LicensedProductsBLAs/BloodDonorScreening/UCM213698.pdf
Medication Deferral Lists http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/LicensedProductsBLAs/BloodDonorScreening/UCM213553.pdf
The Physical Examination • The donor center representative evaluates the prospective donor with regard to • General appearance • Weight • Temperature • Pulse • Blood pressure • Hemoglobin • Skin lesions
Informed Consent • AABB Standards mandates informed consent of allogeneic, autologous, and apheresis donors be obtained. • The donor must be informed of the risks of the procedure and also of the tests that are performed to reduce the risk of infectious disease transmission to the recipient.
DONOR INFORMED CONSENT • Risks of donation • Infectious disease testing • Donor will be informed if test positive • Place on donor deferral list if test positive • Blood may be subject to processing and/or research • Donor has been informed about donation process and had his/her questions answered • Remember: State laws and institutional policies vary, so always become familiar withlocal policies before obtaining patient consent • E.g., in some states, it is a felony to donate blood if you know you are HIV+
Autologous Donors • Most autologous blood is used to treat surgical blood loss in very specific situations where there is a reasonable opportunity to avoid homologous transfusions and/or when compatible allogeneic blood is not available. • Advantages include decreased risk of disease transmission, transfusion reactions, and alloimmunization.
Autologous Donors • Disadvantages of autologous donation/transfusion beyond the usual risks • Bacterial contamination • Circulatory overload • Cytokine mediated reactions and product/recipient misidentification
Methods for Obtaining Autologous Blood • Preoperative collection • Acute normovolemic hemodilution • Intraoperative collection • Postoperative collection
Directed Donation • A directed donation is collected under the same requirements as allogeneic donors, but is directed toward a specific patient. • The tag for the directed unit is a distinct color. • If the donor is a blood relative, the unit must be irradiated to prevent GVHD. • A system should be in place to ensure directed units from blood relatives are irradiated.
Apheresis Collection • A means for collecting a specific blood component while returning the remaining whole blood components back to the patient. • Blood separated into components with centrifugal force based on differences in density. • Can be used to collect large volumes of the intended component, such as platelets, plasma, white cells, red cells, and stem cells.
Apheresis Collection (cont’d) • Donor requirements are generally the same as for whole blood donation, although time intervals between donations can vary depending on the component collected. • Does require a specific informed consent
Apheresis Collections • RBC’s • Plasma • Platelets • WBC’s • Combination of products
Whole Blood Collection • Once the donor has satisfied requirements of the screening process and has been registered, whole blood collection proceeds. • Donor identification • Aseptic technique • Collection procedure • Post-donation instructions
Donor Reactions • Reactions can be divided into three categories • Mild reactions • Moderate reactions • Severe reactions • The donation center staff should also be prepared to properly treat hematomas.
Donor Records • Donor records must be retained by the blood collection facility as mandated by the FDA and AABB. • There must be a system to ensure that confidentiality of the donor is not compromised, and that donor records are not altered.
Donor Processing • The processing tests performed on donor blood include the following • ABO/Rh • Antibody screen • HBsAg • Anti-HBc and NAT • Anti-HCV and NAT
Donor Processing (cont’d) • Anti-HIV-1/2 and NAT • Anti-HTLV-I/II • WNV RNA • Syphilis • T. Cruzi (Chagas Disease) • Platelet bacterial detection
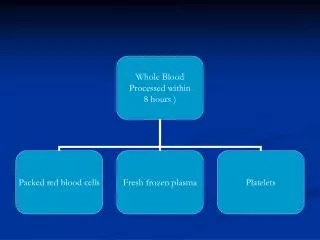
Component Preparation • A single blood donation can provide transfusion therapy to multiple patients in the form of RBCs, platelets, fresh frozen plasma, cryoprecipitate. • The AABB Standards address the preparation, quality indicators, and storage requirements for all component products.
Component Preparation • Whole blood • Red blood cells • RBC aliquots
Component Preparation • RBCs irradiated • RBCs leukoreduced • Frozen/deglycerolized RBCs • High glycerol (40% weight per volume) • Low glycerol (20% weight per volume)
Component Preparation • Platelet concentrates • Platelet aliquots • Platelets leukoreduced • Platelets Irradiated
Component Preparation • Single-donor plasma • Thawed plasma and liquid plasma • Cryoprecipitated antihemophilic factor
Packed RBCs • Approx. 1/2 the volume of Whole Blood • Total Volume: 250-330 ml • Final Hematocrit: <80% for non-additive units and 55-65% for units with additives • CPDA 1 - 35 days closed system • AS-1 - 42 days closed system
RBC Anticoagulant/Preservative Solutions Anticoagulant-Preservative Contents • Citrate: anticoagulant • Dextrose: ATP generation via glycolytic pathway • Adenine: A substrate for RBC synthesis of ATP • Sodium biphosphate: Buffer
RBC Component Storage Lesion • Definition: The biochemical changes that occur during storage of RBC components. • Changes in Red Blood Cells include: • Oxygen dissociation curve shifts to the left • Decreased • #of viable cells • Glucose • ATP • pH • 2,3-DPG • Increased • Lactic Acid • Plasma K+ • Plasma Hgb
Focus mainly on the CPDA-1 and AS-1 anticoagulant- preservative solutions. AABB Technical Manual, 15th Edition, Page 186.
Platelet Components Random Donor Platelets • Prepared from Whole Blood (WB) • Step 1: Maintaining the WB at 20-24oC centrifuge using a Soft Spin (2-3 min at 3200 rpm) • Step 2: Separate platelet rich plasma from RBCs and centrifuge at 22oC using a Hard Spin (5 min at 4200 rpm)
Platelet Components Random Donor Platelet • At least 5.5 x 1010 platelets/unit • Store at 20 to 24oC with continuous agitation • 55-65 ml plasma • pH of 6.0 or greater Single Donor Platelet - Apheresis • At least 3.0 x 1011 platelets/unit • Store at 22 to 24oC with agitation • Suspended in 300 ml plasma • pH of 6.0 or greater
Pooled Platelets • Process of pooling a number of Random Donor Platelets into a central bag. • Pool anywhere from two to twenty units.
Platelet and Plateletpheresis • Dosage Effect: Patient platelet count should increase by 5-10,000 per random donor platelet transfusion and 30-60,000 per single donor platelet transfusion. ABO and Rh Compatibility • Pediatric: Want to transfuse ABO/Rh compatible platelet products.
Plasma Components Fresh Frozen Plasma (FFP) • Frozen at -18oC: • Frozen at -65oC: • Thawed - 150-250 ml total volume • Contains all clotting factors
CryoprecipitatedAntihemophilic Factor (Cryo) • Preparation Procedure • Take FFP (frozen within 8 hrs of collection) from Whole Blood and thaw at 1 to 6oC until it becomes slushy • Then centrifuge plasma using Hard Spin (5-7 min at 3500-4200 rpm). Express plasma leaving approximately 10-15 ml with Cryo. • Refreeze Cryo at -18oC for 12 months
CryoprecipitatedAntihemophilic Factor (Cryo) • Contains at least 80 units of AHF and at least 150mg Fibrinogen • Also contains Factor XIII and vonWillebrands factor
Granulocyte Concentrates • Prepared by Pheresis Should contain 1 x 1010 granulocytes / unit • 200-600 ml plasma and red cells • Store at 20oC to 24oC • Shelf life is 24 hours
Plasma Derivatives • Plasma derivatives are different from blood components because they are prepared by further manufacture of pooled, human source and recovered plasma. • Recombinant DNA technology or monoclonal antibody purification may also be utilized in their preparation.
Plasma Derivatives (cont’d) • Source Plasma is defined as plasma collected by plasmapheresis and intended for further manufacture into plasma derivatives. • Recovered Plasma is plasma recovered from whole blood donations that is shipped frozen to a manufacturer. • Cryoprecipitate is separated from the plasma and used for the production of Factor VIII concentrate.
Plasma Derivatives (cont’d) • The residual plasma is separated into various proteins by manipulating the pH, alcohol content, and temperature. • These products undergo viral inactivation by any of several methods, including heat, solvent-detergent treatment, and nanofiltration.