Download
1 / 71
730 likes | 1.4k Views
Fluid and Electrolyte Abnormalities. Dr. Shreedhar Paudel April, 2009. Water Steady State. Amount Ingested = Amount Eliminated. Body Fluids and Fluid Compartments. The percentage of total body water: 45-75% Intracellular compartment 2/3 of body water (40% body weight)

E N D
Fluid and Electrolyte Abnormalities Dr. ShreedharPaudel April, 2009
Water Steady State • Amount Ingested = Amount Eliminated
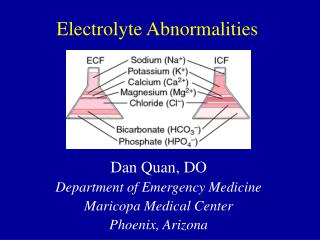
Body Fluids and Fluid Compartments • The percentage of total body water: 45-75% • Intracellular compartment • 2/3 of body water (40% body weight) • Extracellular compartment • 1/3 of body water (20% body weight) • the blood plasma (water=4.5% body weight) • interstitial fluid and lymph (water=15% body weight) • transcellular fluids: e.g. cerebrospinal fluid, aqueous humor (1.5% BW) • Distribution of substances within the body is NOTHOMOGENEOUS
Input TRANSCELLULAR WATER 1% 1 L Body Water Distribution • Individual variability (lean body mass) • 55 - 60% of body weight in adult males • 50 - 55% of body weight in adult female • ~42 L For a 70 Kg man PLASMA WATER RBC ECF 3 L 5% 20% 14 L CELL WATER INTERSTITIAL FLUID COMPARTMENT 40% 28 L 15% 10 L
Goals Review of common electrolyte abnormalities Normal ranges Clinical manifestations of hypo- or hyper- states Causes Treatment options
Hyponatremia Sodium: Normal 135 – 145 mEq / L Symptoms usually begin <120 mEq/L Nausea Lethargy Muscle cramp Psychosis Seizure Coma Death
Hyponatremia Diagnosis based on assessment of serum osmolality and volume status Serum Osmolality Osmolality (calculated) = 2 (Na) + Glucose / 18 + BUN /2.8
Hyponatremia Normal Osmolality (280 – 295 mOsm / kg) Isotonic pseudohyponatremia Hyperproteinemia (>10 mg / dl) Hyperlipidemia (severe)
Hyponatremia High Osmolality (>295 mosm / kg) Hypertonic hyponatremia Hyperglycemia Na: 1.6mEq / liter decrease per 100 mg/dl increase in glucose --Mannitol excess --Glycerol therapy
Hyponatremia Low serum osmolality (<280 mOsm / kg) Hypotonic hyponatremia --Need to assess volume status next in these patients
Hypotonic hyponatremia Hypovolemia GI losses Renal losses plus excess water ingestion Third space losses Tx: Isotonic saline
Hypotonic Hyponatremia Hypervolemia CHF Liver disease Nephrotic syndrome CKD Urine Na: < 20 mEq /liter except in CKD Tx: Salt restriction / water restriction / diuretics
Hypotonic Hyponatremia Isovolemia Glucocorticoid insufficiency Hypothyroidism Psychogenic polydipsia Medications (amitriptyline / cyclophosphamide / carbamazepine / morphine) SIADH Nausea / pain / emotional stress Diuretic use with potassium depletion
Isovolemic Hypotonic Hyponatremia SIADH Syndrome of inappropriate antidiuretic hormone Hypotonic hyponatremia Clinical euvolemia Inappropriately elevated urine osmolality (>200) in face of low serum osmolality Urine Na >20 mEq / liter Normal renal function / TSH / cortisol
SIADH Acute tx Severe hyponatremia (<110 mEq / liter) NS with 20 – 40 mEq / liter KCL IV lasix Rarely 3% saline will be needed Chronic tx Mild hyponatremia Water restriction to approx 1000 ml / day Demeclocycline 300 mg PO bid if water restriction not working (contraindicated in liver disease)
SIADH • Chronic treatment (cont) • Vasopressin receptor antagonists • Conivaptan (Vaprisol) IV prep • 20 mg infusion over 30 min, then continuous infusion of 20 mg/24 hrs • Maximum dose 40 mg/24 hrs • Maximum duration is 4 days
Hyponatremia How fast do we correct it?
Hyponatremia Treatment principles Not too fast (pontine myelinolysis) Symptomatic Initial 1 - 2 mEq / L / hr x two hours, then 0.5 mEq / L / hr Asymptomatic 0.5 mEq / L / hr Max in 24 hours: 10 meq total rise Max in 48 hours: 18 meq total rise
Hypernatremia Sodium: Normal 135 – 145 mEq / l Clinical manifestations Tremors Irritability Ataxia Spasticity Mental confusion Seizures Coma Death
Hypernatremia Cause: Net sodium gain Net water loss
Hypernatremia Volume expansion (net sodium gain) Cause Hypertonic saline / NaHCO3 administration Primary hyperaldosteronism Cushing’s syndrome Tx: Diuretics D5W to replace fluid loss after diuretics
Hypernatremia Water depletion Hypotonic fluid losses
Hypovolemic hypernatremia Treatment Calculate free water deficit TBW (liters) = 0.6 x current total body weight (kg) Desired TBW (liters) = Measured Na (mEq/l) x current TBW / Normal Na Body water deficit (liters) = Desired TBW – current TBW
Hypovolemic hypernatremia If hemodynamic compromise, then replace initially with NS Otherwise use ½ NS or D5W Aim to decrease Na by 0.5 mEq / liter / hr Correct one half of the water deficit in 24 hrs Correct other half over next 24-48 hours
Hypovolemic hypernatremia Diabetes insipidus Sxs: Polyuria / Polydipsia / Low urine osm Central Tumor / Granuloma / Trauma / Surgery Nephrogenic Severe hypokalemia / hypercalcemia / CKD / Drugs (lithium / demeclocycline / amphotericin)
Hypovolemic hypernatremia DI Differentiation of central and nephrogenic Trial of water deprivation Failure to concentrate urine confirms DI Subsequently given arginine vasopressin Central DI (urine concentration increases) Nephrogenic DI (no increase)
Hypovolemic hypernatremia DI Treatment Central Vasopressin 5-10 mcg intranasally per day / bid Nephrogenic Correction of underlying cause if possible Thiazide diuretic / salt restriction can help
Hypokalemia Normal K level: 3.5 – 5.0 MEq/L Clinical manifestations Fatigue Cramps Constipation Weakness / Paralysis Parasthesias Arrhythmias
Hypokalemia EKG abnormalites Flattened T waves ST depressions Prominent U waves
Hypokalemia Causes GI losses Renal losses Acid-base shifts
Hypokalemia Treatment Oral therapy Mild hypokalemia Ability to tolerate oral replacement Increase dietary intake Potatoes / Bananas KCl preparations Can be used in range 8 – 20 mEq/L Monitor K level and adjust dose as needed Correct cause
Hypokalemia Treatment IV repletion Severe hypokalemia Inability to tolerate oral repletion Max Concentration: 60 mEq / liter Rate: 10 mEq / hr Monitor response and decrease concentration or rate as appropriate.
Hyperkalemia Potassium Normal 3.5 – 5.0 Elevated potassium level should be evaluated as to the following: What is the cause? Is the cause an acute or chronic issue? Are there accompanying EKG changes?
Hyperkalemia Symptoms Usually asymptomatic Muscle weakness / paralysis EKG abnormalities Peaked T waves ST depression 1st degree AVB QRS widening “Sine wave sign”
Hyperkalemia EKG changes
Hyperkalemia Think about the cause 1. Too much total potassium Renal disease Intake increased (rare outside of renal disease) 2. Shift of potassium from intracellular space to extracellular space DKA
Hyperkalemia Does the potassium level make sense in the patient? Pseudohyperkalemia
Hyperkalemia When do we treat Patient assessment Cause Chronicity Degree of potassium elevation <6.0 Does not need acute invasive tx >6.0- 6.5 Kayexalate +/- other modalities >6.5 Consider more acute modalities
Hyperkalemia Treatment options Calcium gluconate Regular insulin Albuterol nebulizer treatment NaHCO3 Kayexalate Dialysis
Hyperkalemia Calcium gluconate IV formulation is 1000 mg / 10 ml (10% soln) Dose: Action: Stabilization of cardiac cells. Does not lower potassium. Used for hyperkalemia with EKG changes. If EKG changes do not immediately resolve, dose can be repeated in 5 minutes.
Hyperkalemia Calcium gluconate Precautions Do not infuse with bicarbonate (precipitation of calcium carbonate) Do not use routinely with digitalis as hypercalcemia can augment digitalis toxicity. Limit use to patients with widened QRS.
Hyperkalemia Beta agonist Albuterol nebulizer treatment 2-4 ml of 0.5% soln (10-20 mg dose) Note a usual nebulizer tx for RAD is 2.5 mg Peak effect in 90 minutes
Hyperkalemia Insulin Regular insulin 10 units IV plus one D50 Amp over 5 minutes. This will give patient 25 grams of glucose. Follow this with a D 5 containing IV maintenance fluid for several hours. Effect within 15 minutes. Peak effect 60 min. Duration 3-4 hours.
Hyperkalemia NaHCO3 1 Amp (44.6 meq) IV over 5 minutes. Onset: 30 minutes Duration: 60-120 minutes
Hyperkalemia Kayexalate (Na – K exchange resin) PO dosing: 15 -30 gram Can be used as a dry powder Can be mixed with 60-120 ml of a 20% sorbitol soln to avoid constipation PR dosing: 50 grams Mix with 50 ml of 70% sorbitol and 100 ml tap H20 Retain in rectum x 30 minutes minimum but ideally 2+ hours
Hypocalcemia Normal Calcium: 8.9 – 10.3 mg/dl Calcium 40% bound to albumin 15% bound to other serum anions 45% is ionized in serum
Hypocalcemia Correct for low albumin 0.8 mg / dl drop in Calcium for every 1 g / dl drop in Albumin Corr Ca = Meas Ca + (0.8 * (4.5 – Meas Alb))
Hypocalcemia Clinical signs of low calcium: Tetany / Carpopedal spasm Trousseau’s sign Chvostek’s sign Lethargy / confusion Seizures Heart failure
Hypocalcemia Treatment of symptomatic cases Calcium gluconate (10% soln) which contains 100 mg elem calcium / 10 ml. 1. Give two ampules IV over 10 minutes then 2. Add six ampules to 500 ml D5W and infuse at 1 mg / kg / hr