Download
1 / 25
250 likes | 381 Views
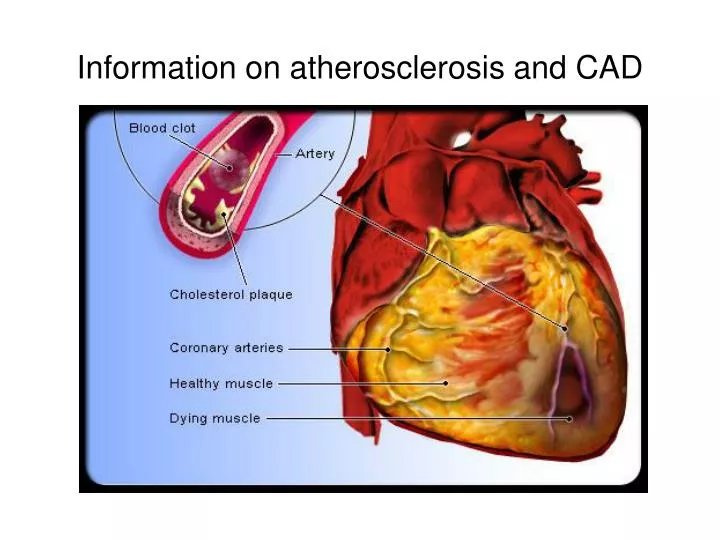
Information on atherosclerosis and CAD. How is Coronary Artery Disease Diagnosed?. Alternatives to bypass surgery. Methods to perform bypass surgery. Methods to perform bypass surgery. Methods to perform bypass surgery. Ascending aortic disease.

E N D
Methods to perform bypass surgery Ascending aorticdisease
Evolution of Minimally Invasive Bypass 1990’s 2000’s Present On-pump bypass Off-pump bypass Minimally Invasive (OPCAB)
Liberal use of BIMA R Poston: 45% use Srivastava: 150 cases1 National average2: 6% Boston average3: 4% EndoACAB4: 5.3% Long-term Results for Robotic Bypass Two IMAs are better than one5 • Srivastava, Ann Thorac Surg. 2006;81(3):800-6 • Circulation 2009;120(11):935-40 • MASS-DAC report, 10/14/09 • Vassiliades, Ann Thor Surg 2007; 83:979-84 • Lytle BW et al. JTCVS 1999;117:855-72
Possible Complications • Failure of the bypass grafts • Conversion to an open procedure (1-2% risk) • Unable to tolerate breathing with one lung • Poor access to the arteries that need to be bypassed • Bleeding that can not be controlled • Incisional pain • Learning Curve
Candidates for Robotic Bypass • Suitable coronary arteries for bypass • Able to tolerate breathing with one lung • No evidence of unstable symptoms or blood pressure
How to reach Dr. Poston • Office phone: 773-702-2500 • Cell phone: 617-610-0126 • Email: rposton@surgery.bsd.uchicago.edu • Address:Robert Poston, MDProfessor of SurgeryDivision of Cardiothoracic SurgeryUniversity of Chicago Medical Center5841 S. Maryland Ave, MC 5040Chicago, IL 60637Fax 773-702-4187
What Happens During a Consultation?Review of Coronary Angiographic Images Discrete blockage, good targets Multiple blockages, poor targets
What Happens During a Consultation?Review of Medical History • No contraindications for surgery and general anesthesia • Appropriate need for bypass surgery (vs. stenting or medical therapy) • Appropriate candidate for less invasive approach • Stable symptoms • Adequate lung function
Quicker recovery Less complications Sternal infection Stroke Reduced loss of blood, fluid, heat during surgery Long-term results not yet confirmed Safety compromised in certain patients Unexpected events occur during the “learning curve” What Happens During a Consultation?Review of Pros and Cons of Robotic Bypass
What Happens During a Consultation?Why wasn’t this option brought up before? 1) For many patients, robotic bypass as an appropriate option for the treatment of CAD 2) Traditional bypass surgery is not clearly more effective in all respects that matter to patients. 3) The choice between available options is sensitive to the preferences of individuals 4) Clinicians often make assumptions about patients’ preferences and provide recommendations without explaining all options.
Testing required before surgery • Lung function (if necessary) • Other organ function (liver, kidneys, brain) • Clotting tests • Any prior problem with surgery? • Is there a pacemaker? – EP consult • Consultation with anesthesiologists
Day of Surgery • Arrive at the Admitting Department for check-in (6am for first case, 10am for second case) • Will be escorted from Admitting to Preop Holding Area. • Dr. Poston will visit you and family in Preop Area at 6:45am • Taken to OR at 7:00am • After the case is complete (typically 12noon to 2pm) • Patient will go to CTICU • Dr. Poston will immediately contact family to discuss case • If case extends beyond 3pm, nurse on team will contact family to provide update • If no update provided or any other concern, call Dr. Poston’s cell phone 617-610-0126 • For interested family, best means for information from Dr. Poston is via email: rposton@surgery.bsd.uchicago.edu (allow 4-6 hour timeframe for response) • Dr. Poston will contact your primary care provider and cardiologist within 24 hours via telephone to provide update
Events After Surgery • Typical length of stay in the CTICU is 12 to 36 hours, which depends mainly on: • Stable blood pressure • Adequate urine output • No bleeding or need for transfusions • Breathing comfortably without the need for assistance other than nasal cannula • Adequate pain control • Once cleared, will be transferred to a “step-down unit” until ready for discharge to home which depends mainly on: • Able to walk steady without assistance • No requirement for nasal cannula to maintain oxygen levels • No other outstanding medical issues • Dr. Poston will the patient in the CTICU twice a day at 6:45am and 4-5pm and when in the step-down unit once a day at 7-8am. • For primary contact person, if no update provided prior to discharge or any other concern, call Dr. Poston’s cell phone 617-610-0126 • For interested family, best means for information from Dr. Poston is via email: rposton@surgery.bsd.uchicago.edu (allow 4-6 hour timeframe for response) • Dr. Poston will provide your primary care provider and cardiologist with a copy of the discharge summary and operative note via fax and letter
Events After Discharge • Typical length of recovery (i.e. time to return to work or normal activity) is 3 weeks, which depends mainly on: • Physical functioning that was possible prior to surgery • Degree of activity that is required for your job • Presence of surgical complications that would delay your recovery • Whether your pain is well controlled • At 3 weeks, outpatient clinic visit will be scheduled. Purpose of this visit is to check the healing of the wounds and assess for any complications. • If any problems arise before clinic visit, call Dr. Poston’s cell phone 617-610-0126 or contact via email: rposton@surgery.bsd.uchicago.edu (allow 4-6 hour timeframe for response) • Dr. Poston will provide your primary care provider and cardiologist with a copy of the clinic note describing your status at the follow-up visit.
Follow-up test after bypass surgery RIMA LIMA LAD OM1 Predischarge CT angiography
Concerning Symptoms After Discharge • Chest pain • Not concerning if located near incision and pain is made worse by coughing or putting pressure on incision • Concerning if similar to symptoms that were present prior to undergoing bypass surgery • Wound problems • Redness, worsening pain, swelling • Excessive drainage • Breathing difficulties that get progressively worse rather than better • If any problems arise before clinic visit, call Dr. Poston’s cell phone 617-610-0126 or contact via email: rposton@surgery.bsd.uchicago.edu (allow 4-6 hour timeframe for response)