Download
1 / 25
250 likes | 296 Views
Practical Aspects of Nutrition Support in the ICU. John W. Drover, MD, FRCSC, FACS Associate Professor Queen’s University Kingston, ON Canada. www.criticalcarenutrition.com. Disclosure Information. None. www.criticalcarenutrition.com. Objectives.

E N D
Practical Aspects of Nutrition Support in the ICU John W. Drover, MD, FRCSC, FACS Associate Professor Queen’s University Kingston, ON Canada www.criticalcarenutrition.com
Disclosure Information • None www.criticalcarenutrition.com
Objectives At the end of the session the participant will be able to: • List 3 strategies to maximize the benefits of enteral nutrition. • List 2 advantages of post-pyloric enteral feeding. • Identify 1 method of gaining post-pyloric access at the bedside in the ICU.
Outline • Review the rationale for enteral feeding. • Focus on the data regarding post-pyloric feeding. • Specifically RCT’s • Clinically important outcomes • Review the risks of and obstacles to post-pyloric feeding. • Develop a recommendation www.criticalcarenutrition.com
Case #1 • Day #1 • 50 yo female COPD with CAP • Intubated, resuscitated • Who would start EN within 24 hours of admission? • Who would attempt to place a post-pyloric feeding tube?
Case #2 • Day #5 • 50 yo female COPD with CAP • Intubated, resuscitated • feeding tube in stomach • Receiving metoclopromide • Achieving <30% of goal; GRV >400ml • Who would recommend placement of a post-pyloric feeding tube?
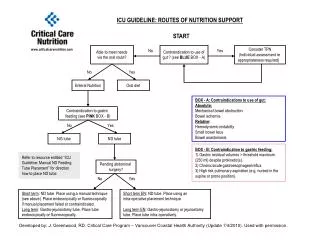
Nutrition in the Critically ill • Enteral nutrition strongly recommended • Early enteral nutrition recommended • Optimize the benefits and minimize risks • Use of feeding protocols • Motility agents for gastric feeding • Small bowel feeding
Intra-gastric feeding The good: • Easy access • Early initiation • Often tolerated well The bad: • Gastric residual volumes (GRV’s) • Gastro-pharyngeal reflux • Respiratory aspiration • Unrealized nutritional goals
Post-pyloric feeding 2 RCT’s that have evaluated aspiration • 33 patients, 1st 3 days • GE regurg 24.9% vs. 39.8% (p=0.04) • Further into small bowel less aspiration • 54 patients, twice weekly • Low rate of aspiration • 7% vs 13% aspiration Heyland et al, CCM, 2001 Esparaza et al, Int Care Med, 2001
Post-pyloric feeding • 11 RCT’s of SB vs Gastric feeding • Med/Surg (4), Med (3), Trauma (2), Neuro (2) • N=664 • One study used arginine containing diets • Variable design for selection • Different methods of enteral access • Outcomes • No difference in mortality, LOS, vent days Heyland et al, JPEN 2002
Post-pyloric feeding • Taylor et al. CCM, 1999 • Neurotrauma, n=82 • Standard gastric feeding • 15ml/h increase Q8h • Aggressive SB feeding (when feasible) • SB access only 34% • Start at target rate and adjust • Outcomes • Pneumonia 44% vs 63%(NS)
Post-pyloric feeding Nutritional outcomes • Small bowel feeding associated with • Reaching nutritional goals sooner • Better success at meeting goals • Meta-analysis not possible • Variable gastric feeding strategies • Goals and success reported in different ways
Post-pyloric feeding • Infections – pneumonia (9 studies) • 8 clinical criteria; 1 bronchoscopy • SB feeding associated with reduced pneumonia • RR=0.77(0.60-1.0), p=0.05 • 23% risk reduction • With Taylor study removed • RR=0.83(0.6-1.15), p=0.3
Controversy “A comparison of early gastric feeding in critically ill patients: a meta-analysis” • No difference in outcomes • Same RCT’s • Exclude Taylor • Use studies of reflux • Didn’t count all pneumonia in Montecalvo study Ho et al, ICM 2006
Post-pyloric feeding • Problems associated with: • Difficult to achieve • Once achieved may move • Doesn’t overcome all issues • (eg. ACS, short bowel, enteric fistula) • Bowel necrosis – rare event not clearly associated with enteral nutrition Canadian survey says 10% Safe Zaloga: Nutrition Week 2005
The ENTERIC Study The Early Nasojejunal Tube To Meet Energy Requirements In Intensive Care Study Study Investigators: Andrew R Davies Rinaldo Bellomo D Jamie Cooper Gordon S Doig Simon R Finfer Daren K Heyland For the ANZICS Clinical Trials Group
Conclusions • SB feeding improves • time to reach target goals • success at achieving target goals • SB feeding may be associated with less pneumonia
Discussion • Routine use: • Difficulties of SB access • Blind • Endoscopic • Flouroscopic • Patients with gastric intolerance • Patients with other risk factors • GERD • unable to nurse semi-recumbent • (eg. C-spine injury)
Discussion • If your unit has feasible access • Go for it • If your unit has ability with effort • Use it for patients at risk • i.e. inotropes, sedatives, paralytics, high GRV’s • If your unit has great difficulty • Use in patients who do not tolerate gastric feeding
Bedside placement into SB • Feeding tube in stomach • Wire with 30o bend, 3cm from end • Zaloga, Chest 1991 • Insufflate stomach with ~500ml • Salasidis, CCM 1998 • Rotate while advancing • Samis and Drover, ICM 2004
Thank You! • Choosing an approach to: • MAXIMIZE BENEFIT • Minimize risk