Download
1 / 58
590 likes | 609 Views
Explore how the Abbreviated Injury Scale (AIS) and Injury Severity Score (ISS) are crucial tools for evaluating trauma outcomes, survival rates, and severity. Learn about AIS coding, ISS calculation steps, and the importance of detailed injury information. Get insights into the AIS system and its evolution, including AIS2005 and AIS2015 updates. Discover how injury location, type, and severity impact ISS scoring and patient prognosis. Stay informed about trauma assessment advancements with the TARN network.

E N D
Measuring Trauma OutcomesInjury Severity Score (ISS)Probability of Survival (Ps17)Hospital Survival rate (Ws)BOAST4Chest Wall Injury reportThe Trauma Audit & ResearchNetwork (TARN)
Injury Coding • Injury coding performed centrally at TARN • Ensuring coding uniformity • Coders check injury descriptions & imaging reports • Abbreviated Injury Scale dictionary (AIS2005) currently used • Every submission assigned an Injury Severity Score (ISS) • 75,000 submissions per year coded
Abbreviated Injury Scale: AIS • THE Internationally recognised system for injury scoring • Produced by AAAM (Association for the Advancement of Automotive Medicine)in U.S.A • Introduced in 1970, originally for Vehicle Crash investigators • AIS2005 version >2000 injury descriptors • Anatomically based system, ranking injuries according to severity on a 6 point ordinal scale
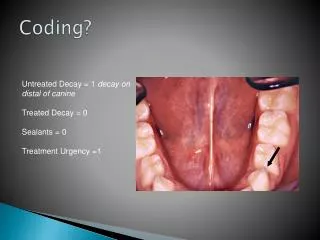
AIS Severity indicates The relative risk of “threat to life” in an average person who sustains the coded injury as his or her only injury It’s not a disability scale
AIS: Spinal Injuries • Cervical Spine (C1-C7) • Thoracic Spine (T1-T12) • Lumbar spine (L1-L5) Severity can be affected by location of spinal injury
AIS: Confirmed injuries only Suspected injuries Possible injuries Probable injuries Ruled out injuries
AIS: Not Coded • Infections • Pneumonia • Death • Blindness • Miscarriage • Epilepsy following head injury • Pulmonary embolism following skeletal injury • Don’t affect Severity score
NFS: Not Further Specified This appears throughout the AIS dictionary & allows the coding of injuries when detailed information is lacking Example: Injury description = Liver laceration Coded as: 541820.2 (Liver laceration NFS)
AIS 6: Maximum score AIS 6 not used just because a patient dies! • Has to be documented medical evidence of an AIS 6 injury
AIS 6: Maximum score • Head or Neck • Brain stem: laceration, crush, penetrating or transection • C3 or higher complete cord transection or contusion • Sigmoid or Transverse sinus or Internal carotid artery: Bilateral lacerations • Thorax • Heart: rupture, multiple lacerations or avulsion • Total chest crush • Aortic rupture + haemorrhage not confined to mediastinum • Bilateral pulmonary artery or vein transection • Severe inhalation • Abdominal & Pelvic contents • Liver avulsion • External • 2nd or 3rd degree burns > 90% Total Body Surface • Massive Whole body Explosion type injury
AIS: Localisers • 2 additional localiser codes, allow coding of: • Localiser 1 Side or aspect of an injury • e.g. Right, left, Upper, Temporal, Frontal • Localiser 2 Actual Site of an injury • e.g. 5th rib, 12th Thoracic vertebrae, 2nd toe • Don’t affect ISS • Used mainly in Research
AIS dictionary • Available only from: www.aaam.org • Latest Version: AIS 2015 recently released • $225 each + shipping • TARN will moving to AIS2015 at end of year • All existing codes will be mapped over • All Trusts notified well in advance
853251.3 752372.3 856164.5 450203.3 140626.5 150400.2 544224.3
Calculating the ISS Injury Severity Score
Calculating the ISS: Step 1 Determine the scores of the individual injuries using the Abbreviated Injury Scale
Calculating the ISS: Step 2 • Identify the highest severity score in each body area
Injury Severity Score: 6 body areas • Head & Neck & Cervical spine • Face • Chest & Thoracic spine • Abdomen & pelvic contents & Lumbar spine • Extremities & bony pelvis • External (incl. Skin injuries and Burns)
Calculating the ISS: Step 3 • Square the highest score in each body area
5² =25 3² =9 3² =9 5² = 25
Calculating the ISS: Step 4 • Code individual injuries • Identify the highest score in each body area • Square the highest score in each body area • Add together the highest AIS2 from 3 different body areas
5² =25 3² =9 3² =9 5² = 25
Injury Severity Score • (ISS) = 59
Injury Severity Score (ISS) 2² = 4 2² = 4 ISS = 8
Injury Severity Score (ISS) 2² = 4 2² = 4 1² = 1 ISS = 9
Injury Severity Score (ISS) • Ranges from 1 to 75 • Maximum 75 achieved in 2 ways: • Severity 5 in 3 different body areas • 52 + 52 + 52 = 75 • ISS convention: • AIS = 6 in any body area, ISS = 75
Importance of Injury Detail • Length, depth or Grade of lacerations (especially to internal organs) • Depth, size and location of haemorrhages and contusions (especially in the brain) • Open or Closed fractures • Stability & site of Fractures (e.g. Comminuted/Displaced Shaft/Proximal/Distal fracture) • Articular (joint) involvement (e.g. Intra-articular, extra-articular) • Blood loss • Vessel damage • Location & number of rib fractures • Compression or effacement of ventricles/brain stem cisterns • Neurology associated with spinal cord injuries • Grade, Instability, Blood loss or Vascular damage associated with Pelvic Fractures • Cardiac arrest associated with asphyxia or drowning • Ensure all injuries are documented • Include imaging reports or Post Mortems for every submission. • Jan 17: Grade now requested for pelvic ring fixations
Probability of Survival Once ISS is assigned Probability of Survival (Ps) calculated eachsubmission
Why calculate PS? • Need to assign weight to deaths and survivors. • Some deaths more statistically significant than others. • Case mix adjustment. • Performances measurement: hospital and networks.
Ps history • TARN developed first Ps model in 2004 • Remodelled in 2007, 2009, 2012, 2014 and 2017 • Components used in Ps since 2014 (best predictors of outcome): • ISS • Age • Gender • GCS • Pre-Existing Medical Conditions (PMC) • Charlsoncomorbidity index adds ‘weighting’ PMC
Ps17 (launched July 17) * *Charlson index (1984, revised).
What is Ps? PS% is retrospective measure of pts with same profile on TARN database. TARN database: past 4 years (Approx 300,000 cases) Ps = 63%, then 63 out of every 100 patients with that profile have previously survived. 37 out of every 100 patients have previously died.
Probability of Survival Ps is calculated using: GCS taken on arrival in ED at first receiving hospital where unavailable Pre Hospital GCS where unavailable Presence of Intubation/ventilation where unavailable Impute a “probable” GCS (equivalent weighting)
Ps17 Weighting groups Pre-Existing Medical Conditions
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Weightings for Age, GCS, Gender & PMC
Ps17 Importance of accurate injury detail
Ps17 Importance of accurate injury detail
PS breakdown: shown on website & clinical reports (more later) • Ps Bandings • No. of patients in each band • Observed/Actual survivors • Expected survivors (compared to TARN database) • Difference = Observed – Expected x 100 • No. in group • Ws = Difference x fraction of patients on database in each band Hospital Survival Rate= 0.67 additional survivors per 100 patients 95% Confidence interval Ws lies between this line
Individual Hospital Survival Rateshown on website: English & Welsh sites only +1.2 Survivors Statistically significant outcome (+0.39 to +1.97) +1.2 Survivors Not Statistically significant (-1.83 to +4.2)
Comparative Survival rate (Ws) shown in Clinical report: All hospitals Your hospital 95% confidence intervals
Funnel plots: Potential outlier (positive) Normal range All hospitals Greater Precision: More cases (more reliable) Lower Precision: Fewer cases (not as reliable) Hospitals shown by Precision (no. of cases) Ws must always be viewed in conjunction with Case ascertainment