Download
1 / 47
540 likes | 897 Views
Robert Gosselin MT (ASCP), CLS. von Willebrands Disease. von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA) ( Hemophilia 2008; 14:171-232 )

E N D
Robert Gosselin MT (ASCP), CLS von Willebrands Disease
von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA) (Hemophilia 2008; 14:171-232) von Willebrand Factor Assays: Guideline – Second Edition (H51-2) (in progress)
1924 Erik vonWillebrand evaluated a 5 year old girl with bleeding diathesis and ultimately 66 family members in Finland and noted: • Mucocutaneous bleeding • Autosomal inheritance • Prolonged bleeding times • Normal clotting times • Not corrected with blood transfusions
In 1950 plasma protein defect causing prolonged bleeding time Deemed “von Willebrand factor” As cryoprecipitate and F8 concentrates were produced, it was noted that they complexed together
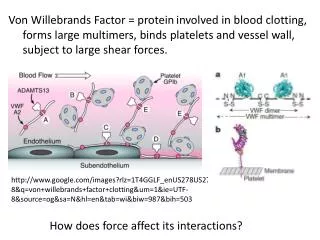
VWF produced in two areas endothelium – synthesized and stored in Weibel-Palade bodies megakaryocytes – stored in alpha granules Assembled from identical subunits to form linear strings multimers formed in the Golgi complex
In circulation, VWF travels as a complex with F8 Upon injury, VWF undergoes conformational change and adheres to the subendothelium under high shear conditions Platelets adhere via GPIb-IX Half-life is ~12 hours
VWF multimers – Degradation by ADAMTS13 [A Disintegrin-like And Metalloprotease domain with ThromboSpondin type 1 motif, member 13] Deficiency of ADAMTS13 have been associated with TTP
VWF functions Hemophilia 2008; 14:177
von Willebrands Disease Plasma protein defect of vonWillebrands factor (vWF) Quantitative defect Partial deficiency type 1 Total deficiency type 3 Qualitative defect (type II) Functional aberration Short arm of chromosome 12
von Willebrands Classification • Type 1-autosomal dominant • Type 2-autosomal dominant • 2A (some autosomal recessive) • 2B • 2M • 2N (autosomal recessive) • Type 3 (autosomal recessive) • Pseudo-type VWD-autosomal dominant • Acquired VWD
von Willebrands Disease 1% of population with vWF • 125/1,000,000 with significant bleeding • In UK, 6294 registered vWD patients, but only 10% received treatment in calendar year 2001 Type I accounts for ~75% of all vWD Dx Mild to severe • Hx • Easy bruising • Nose bleeds • Oral cavity bleeding • Menorrhagia Bleeding variability • Mild to severe
Terminology • VWD –von Willebrand’s disease • VWF - mature von Willebrands protein • VWF:RCo - ristocetin cofactor activity, measures vWF protein activity ** • VWF:Ag -VWF antigen • VWF:CB -collagen binding assay, another component of vWF function • FVIII:C -factor VIII activity • VWF:FVIIIB -vWF-factor VIII binding assay • RIPA -ristocetin induced platelet aggregation • VWFpp -vWF propeptide Hemophilia 2008; 14:177
Basic (recommended first tier) testing • Screening tests • PT and aPTT • PFA (Siemens)* or Plateletworks (Helena Labs)* • NOT bleeding time • VWF:RCo – measures activity • Ristocetin driven • Ristocetin independent • VWF:Ag – measure protein • VWF:RCo/VWF:Ag ratio • F8 – to r/o type 2N * May miss some VWD subtypes
Second tier (subsequent) • Multimer analysis – in suspected type 2 • Ristocetin aggregation • Low dose (0.6mg/ml) • VWF:CBA – in suspected type 2 • VWFpp – in suspected type 1 variants • Other • DDAVP (desmopressin) challenge • IV or nasal • Molecular analysis • Antibodies • Acquired
Factors affecting VWF levels • Exercise • Stress • Psychological • Physiological • Prolonged tourniquet time • Diet?? • Other • Pregnancy, oral contraceptives, HRT • Trauma • Inflammatory process
Other factors influencing VWF levels • Sample type • 3.2% sodium citrate preferred • ABO blood group VWF:Ag mean (range)** • Type O: 75 (36-157) • Type A: 106 (48-234) • Type B: 117 (57-241) • Type AB: 123 (64-238) • Using filters to achieve PPP ** Hemophilia 2008; 14:177
Conjugated Anti-human VWF antibody ¤ VWF (+) Chromogenic tag Wash Wash Microwell containing anti-VWF ¤ + ¤ Color + ¤ + ¤ ¤ ¤ + + + + + + Amount of color proportional to amount of antibody present Incubate Incubate ELISA and LIA based testing Reagent beads coated with anti-vWF Patient vWF Instrument reading—changes in optical density secondary to aggregates Incubate Testing well
Results compared to Std curve Platelet agglutination and aggregation testing Patient’s plasma + Ristocetin Ristocetin 1.2 mg/mL (l) & 0.6 mg/mL (r) Patient’s platelets & plasma + Ristocetin Results compared to normal population Zhou and Schmaier Am J Clin Pathol 2005;123:172-183
VWF:RCo • Platelet poor plasma • Stabilized platelets • Commercially prepared • May be combined with ristocetin • Ristocetin • Initially used as antibiotic • Peptide from Amycolatopsis lurida • Thought to mimic shear effect of shear stress
Problems associated with VWF:RCo Variability • Between lots of ristocetin • Between reagent methods Imprecision not ideal (up to 15%) Low level sensitivity • Automated methods lower limit 15-20%
VWF activityRistocetin independent • Platelet poor plasma • Latex bead coated with monoclonal antibody (anti-GPIb) • Recognizes functional domain of VWF • LIA and ELISA method • May reduce variability associated with VWF:RCo
VWF:RCo vs RIPA VWF:RCo Measures vWF activity Exogenous PLTs Exogenous ristocetin Platelet agglutination ELISA methods (VWF:Act) LIA methods (VWF:Act) RIPA Measures interaction between vWF and platelet GPs Patients plasma Patients platelets Exogenous ristocetin Platelet aggregation vWF:RCo measures plasma vWF only, while RIPA measures both plasma vWF and vWF interaction with platelets
VWF:Ag • Most labs use either ELISA or LIA testing • ELISA testing…hours • LIA testing…minutes • Traditional method is gel electrophoresis • Less variability than VWF:RCo • Possible prozone effects with automated methods (LIA) • Test may be used for other indications • Vasculitis Rx
VWF:CB • ELISA method • Plate coated with type I or type III collagen • Equine-bovine source • Better correlation with HMW vWF • Better reproducibility than vWF:RCo • Improved detection at lower levels • No FDA approved kit in US • Bummer!!!
Collagen binding assay Ratio: vWF:Ag to vWF:CB Favaloro, Am J Clin Pathol 2000;608-618 Type 1 VWD Type 2 VWD
Multimeric analysis of vWF-type II Favaloro, Thromb Haemost 2007; 98:346-358
vWF propeptide (vWF:pp) • Stored in α granules or Weibel-Palade bodies • After secretion into plasma, t½: 2-3 hrs • vs mature vWF t½: ~10 hrs • Plasma concentrations ~1μg/mL • vs mature vWF: 10 μg/mL • Studies suggest: • Increased vWF:pp to vWF:Ag ratio with reduced vWF:Ag true genetic defect with vWF survival • vWF survival would also suggest alternative Rx strategies
Pseudo-VWD • Similar to type 2 • Decreased PLT count • “Gain in function” • Aggregation with low dose ristocetin • Must perform VWF:PB • Increased with VWD:2B • Normal with psuedo-VWD • Abnormal GPIb receptor
CLSI Guideline H51-2 • Recommendations for • Sample type, processing • Testing • Calibration and results reporting • Same calibrator for VWF:Act and VWF:Ag • Different calibrator for therapeutics • Units • Ratios • Implementation/validation proposals?? • Implementing new method • Lot-to-lot
Type I vWD • Hx significant for mucocutaneous bleeds • vWF:RCo, vWF:CB, vWF:Ag are <50 IU/ml • vWF:RCo/vWF:Ag ratio >0.7 • Normal PLT count • Normal multimeric analysis • Factor VIII activity normal/ • Decreased RIPA • PFA C.T. usually , BT slightly better than coin • Propeptide survival??
Type 2A vWD • Qual variant with PLT-dependent function with absence of HMW multimers • Two groups of mutations • Group 1: defective intracellular transport, retention of large multimers in ER • Group 2: enhanced susceptibility to proteolysis of vWF, of large multimers • Missense, deletions, insertions • Clinical Hx (personal or familial) mucosal bleeding
Type 2A vWD • Laboratory finding • Normal PLT count • Decreased vWF:RCo • Decreased vWF:CB • Normal/ factor VIII activity • vWF:Ag usually normal/ • Ratio of vWF:RCo or vWF:CBA to vWF:Ag is <0.7 • RIPA is reduced • PFA C.T. usually • Absence of high molecular weight multimers
Type 2B vWD • Qual variant with “gain of function” • Increased affinity for for platelet GpIb • 4 mutations (nucleotide substitutions) within the vWFA1 domain account for ~90% of type IIb • Similar laboratory parameters as pseudo-type vWD • Clinical Hx (personal or familial) mucosal bleeding
Type 2B vWD • Laboratory finding • Normal to slightly PLT count • Decreased (usually) vWF:RCo • Decreased (usually) vWF:CBA • Normal/ factor VIII activity • vWF:Ag usually normal/ • Ratio of vWF:RCo or vWF:CBA to vWF:Ag is <0.7 • RIPA is • low dose of ristocetin (0.75 mg/mL) • PFA---normal to • Absence of high molecular weight multimers
Pseudo-type vWD • Mutations in GpIb-IX complex on platelet surface • Variable clinical bleeding • Similar laboratory parameters as type 2B: • Variable thrombocytopenia • Enhanced RIPA • Decreased HMW multimers
Differential Lab Dx: Type IIb versus Psuedo type vWD • Normal PLTs to type IIb sample: • Enhanced RIPA • Normal Cryoprecipitate to pseudo-type vWD • Spontaneous aggregation VWF:PB assay preferred/definitive
Type 2M vWD • Qual variant with PLT-dependent function without absence of HMW multimers • Missense, small frame delections • Clinical Hx (personal or familial) mucosal bleeding
Type 2M vWD • Laboratory finding • Normal PLT count • Decreased vWF:RCo • Decreased vWF:CBA • Normal/ factor VIII activity • vWF:Ag usually normal/ • Ratio of vWF:RCo or vWF:CBA to vWF:Ag is <0.7 • RIPA is reduced • PFA C.T. usually • Presence of high molecular weight multimers • increased amounts may be seen
Type 2N vWD • A qualitative defect resulting in decreased vWF:FVIII binding • Autosomal recessive • Heterozygotes with normal factor VIII • Bleeding Hx related to surgery or trauma
Type 2N vWD • Laboratory finding • Normal PLT count with prolonged aPTT • Normal vWF:RCo • Normal vWF:CBA • factor VIII activity (usually between 5-30 IU/ml) • Decreased vWF:FVIIIC binding • vWF:Ag normal • Ratio of vWF:RCo or vWF:CBA to vWF:Ag is >0.8 • RIPA is normal • PFA C.T. normal • Multimer pattern is normal
Type III vWD • A virtual absence of vWF protein • Presentation early in life • Multiple mutations, including frame shifts and nonsense mutations, as well as deletions
Type III vWD • Laboratory finding • Prolonged aPTT • Absence of vWF:RCo • Absence of vWF:CBA • Markedly factor VIII activity • Absence of vWF:Ag • RIPA is markedly abnormal • PFA C.T. markedly abnormal • No detectable multimer pattern