Download
1 / 51
580 likes | 841 Views
Avoidant Restrictive Food Intake Disorder: Overview of typical presentations and treatment. Date: 09/11/2019 Speaker(s) Name: Finza Latif, MD and Rebecca Begtrup , DO MPH Speaker(s) Disclosure information: No relevant financial relationships to report Talk Title:

E N D
Avoidant Restrictive Food Intake Disorder: Overview of typical presentations and treatment Date: 09/11/2019 Speaker(s) Name: Finza Latif, MD and Rebecca Begtrup, DO MPH Speaker(s) Disclosure information: No relevant financial relationships to report Talk Title: Learning Objectives: 1. Learn about the diagnostic criteria for ARFID; 2. Learn about treatment options 3. Highlight differential diagnosis, relevant psychiatric and medical comorbidities and potential diagnostic pitfalls. Commercial Support for this activity has been provided by: ‘None’ CME Accreditation George Washington University Hospital is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Credit Designation Georgetown University Hospital designates this live activity for a maximum of 1.5AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Restrictive Eating Disorders: An INTERACTIVE update on diagnosis and evidence based treatments Rebecca Begtrup, DO MPH Clinical Instructor of Psychiatry Children’s National Health System FINZA LATIF, MD Assistant professor of psychiatry Director of consultation liaison service CHILDREN’S NATIONAL HEALTH SYSTEM
DSM V • “Feeding & Eating Disorders of Infancy & Early Childhood” and “Eating Disorders” combined to “Feeding and Eating Disorders”. • DSM-IV’s “Feeding and Eating Disorders of Infancy and Early Childhood” -> DSM-V’s “Avoidant Restrictive Food Intake Disorder” • Expanded the diagnostic criteria to acknowledge the continuation of these disorders into adolescence & adulthood.
Diagnostic Criteria: ARFID • An Eating or Feeding Disturbance… • Apparent lack of interest in eating or food • Avoidance based on sensory characteristics of food (texture, consistency, temperature, smell) • Concern about aversive consequences of eating (such as fear of choking) • …Causing persistent failure to meet appropriate nutritional/energy needs as manifested by 1 or more of: • significant weight loss, failure to achieve expected weight gain, or faltering growth in children • significant nutritional deficiency • dependence on enteral feeding or oral nutritional supplements • marked interference with psychosocial functioning
“Picky Eater” Presentation Types PHOBIA Sensory
Diagnostic Criteria Cont’d • B: Not due to a lack of available food or due to a culturally sanctioned practice. • C: Does not occur exclusively during AN or BN and there is NO body image disturbance. • D: Not due to another medical or psychiatric disorder. • When it occurs in context of another condition, it exceeds that which would routinely be associated w/this condition & warrants additional clinical attention.
Differential Diagnosis • Other medical conditions • GI disease, food allergies, malignancies • Specific neurologic/neuromuscular, structural, or congenital d/o’s & conditions associated w/feeding difficulties • Conditions w/associated oral/esophageal/pharyngeal structural or functional problems –hypotonia, tongue protrusion, unsafe swallowing • Reactive attachment disorder • Withdrawal of child leads to child-caregiver relationship disturbance -> can affect feeding • Child abuse or neglect • As well as parental psychopathology • Autism spectrum disorder • Often present w/rigid eating behaviors & elevated sensory sensitivities
Differential Diagnosis Cont’d • Specific phobia, social anxiety, & other anxiety d/o’s • Specific phobia of vomiting or choking, for example • Anorexia nervosa • Food restriction is accompanied by fear of weight gain or becoming fat OR behaviors that interfere w/weight gain (as these pts may not always admit to fear of wt gain), as well as body image distortions • Major depressive disorder • Appetite may be suppressed & associated wt loss • Schizophrenia spectrum disorder • Odd eating behaviors related to delusional beliefs • Factitious d/o or factious d/o imposed on another • Assumption of the sick role – There may be inconsistencies with the described diets and feeding behaviors
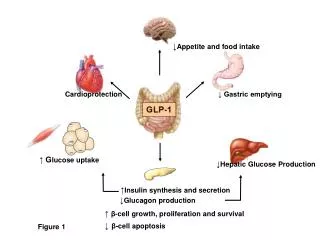
Treatment • Goal is to restore (or create) normalized feeding behaviors in both child and parents (& family) • Therapeutic interventions are primary • Focus on family meals • The What, When, How Much approach to feeding • Ellyn Satter, M.S., R.D, L.C.S.W., B.C.D. • Medications to assist with comorbid sleep, anxiety, & other conditions, if indicated
The 3 Subtypes • Lack of interest (“Infantile Anorexia”) • Avoidance (“Sensory Food Aversion”) • Fear (“Posttraumatic”) • These are 3 distinct disorders diagnostically lumped together into one broader category.
Case Presentation 1- Sam • Sam is a 4 yo CM. His parents report that they are concerned about his eating habits. He is described as a very picky eater with low appetite. • Prefers: hamburgers, chips, french fries, cookies, dry cereal, string cheese on occasion, and creamy peanut butter. • Refuses: all raw vegetables and chewier meats, such as steak or jerky. If finger foods are squishy or messy, he refuses them or insists on his parents feeding him. • Talks during meals • Never says he is hungry. • Gets full quickly • Gags and spits the food out
Sam’s Birth Hx & Feeding Progression • Sam was born full term via SVD; pregnancy and delivery were uncomplicated. • 0-2 months- Exclusively breast fed • 2 months- introduced bottle, formula • 5 months- rice cereal was introduced • 6 months- purees • 9 months- table foods were offered • 9-12 months- only accepted formula • 15 months- crunchy snack foods only. • Throw foods when he was done eating, if kept restrained in the highchair.
Sam’s Current Med Status & Feeding • Current weight = 35 lbs (34.5th %ile) • Current height = 40 inches (8th %ile) • Development: • gross motor skills –on time • fine motor and speech delays noted. • could not tolerate certain textures or smells. • Feeding him “on-the-go”, distractions during meals, only offered preferred foods • His mother quit her job.
Sam’s Nutritional Assessment • A 3 day meal log demonstrated that Sam was taking in only about 45% of the recommended daily allowance for his age, lacking especially in both caloric content and micronutrients. • He was lacking in Vitamin D, Calcium, and had borderline anemia.
Psychiatric Evaluation • Monitored meal and play sessions - monitored from behind a one-way mirror. • During the meal: • Sam ate a few bites before getting up • threw the food & began to cry • During his play session • Sam was calm and focused. • Both parents attended well to his play, and he interacted with both well.
Diagnosis: • Sam suffers from a combination of two subtypes of ARFID: Lack of interest in eating (AKA “Infantile Anorexia”) and Avoidance (AKA “Sensory Food Aversions”).
Symptoms of Lack of Interest in Eating/Infantile Anorexia: All Six Required: • Low appetite, rapid satiety persisting for >/= 1 month • Starting before age 3 years • Does not communicate his hunger & not interested in food (More interested in talking/playing than eating.) • Significant growth deficiency (falling off growth curves) • No traumatic predecessor • Not d/t underlying medical condition
Symptoms of Sensory Food Aversion: All Four Required: • Food selectivity for only certain tastes/textures/smells/temperatures • Onset of selectivity occurred when new types of foods were introduced (ex: move f/purees to finger foods) • Eats preferred foods easily • Lacking of certain micronutrients in his diet and/or oral motor delay (ie: his speech delay 2/2 lagging oral-motor skills 2/2 avoidance of chewy foods)
Treatment: • Tx is complicated by combination of IA and SFA • First step – explain the two-part feeding disorder to Sam’s parents. • At start, offer only foods that Sam • Parents’ foods are “special food” • Tell Sam that his parents will no longer push him to eat their foods, but if he wants to try something, they will give him a small piece.
Treatment Cont’d: • Without Sam, review the Feeding Guidelines with parents. • Enriched formula and vitamin supplementation • Send him to daycare • Return a sense of calm/control • Work on internalizing hunger/fullness regulation. • Later, when he is older and interested, work on increasing the food variety.
Key Feeding Guidelines • Regulate meal times with NO snacking in-between • Family dinners • Small portions of preferred foods • After 1 warning, if behavior repeats, time-out for throwing food or getting up from table • Afterwards, the child returns to the table and parents continue eating
The Full Feeding Guidelines • Feed your child at regular times approximately 3-4 hours apart for 20-30 minutes only. • No other food or drinks, aside from water if thirsty. • Eat all meals and snacks in the kitchen or dining room, rather than in front of the TV or while the child is playing. • Offer your child small portions and allow him/her to have more until he/she is full and does not want to eat anymore. • Occasionally offer your child “special foods” along with the meal (desserts, candies, or “junk” foods). Allow your child to eat these items first, if desired.
The Full Feeding Guidelines Cont’d • Do not praise of criticize your child based on the amount that he/she eats. • Do not use food as a reward, special gift, expression of your affection, or a way to calm your child. Do not restrict food intake or withhold food as a threat or punishment for your child. • Teach your child to sit at the table until “Mommy’s and Daddy’s tummies are full”, rather than leaving when they are “done”. • Discourage your child from playing with the food or talking excessively at the meal. Instead, set a special time for playing and talking with your child after the meal is completed. • If your child gets up from his/her chair, throws food or utensils, or is otherwise misbehaving, give one warning. If the behavior does not resolve, administer a “time-out”.
Case Presentation 2 - Caleb • Caleb is a 9 yo AA M with hx of ARFID (sensory sensitivity subtype) that was successfully treated. • Diagnosed by allergy testing with several food allergies. • NEVER experienced an anaphylactic reaction. • He also has hx of hearing loss and speech delay • Possibly due to the SFA and decreased exposure to chewy foods
Presentation • Caleb was brought to the ED by his parents due to SI and HI. • Reported AH and VH. • Admitted to the child psych unit • 2 months prior to - severe and sudden onset of GERD • Lasted 10 days. • Intense pain and at least one episode of vomiting • Self-imposing an all liquid diet. • Increased anxiety re: food allergies • Behavioral changes • Afraid of swallowing his own saliva • Missed a significant amount of school • Maintained solely on a liquid supplement found online
Initial Inpatient Psychiatric Evaluation • Alert and oriented • Poor historian and avoidant of interaction • N0 abnormal motor movements/tics • Refused to close his mouth completely or allow his lips to touch. • Anxious appearing with mild PMA and poor eye contact. • He appeared his chronological age, but was very thin. • Although bright, he was easily confused and required long periods of time to process questions. No excessive activity or impulsivity was observed. • Mood: “happy”, despite a blunted affect. • Tangential and concrete in his thinking. • Denied SI, HI, SH. • Reported seeing a shadow & hearing a voice • Poor insight, judgement, and impulse control
Vital Signs & Labs • Weight = 25.1 kg (13.2nd %ile) • Height = 130.5 cm (21.3 %ile) • Laboratory values were significant for: hypermagnesemia, hypokalemia, and low prealbumin levels. • The remainder of his chemistries, cholesterol panel, and UTox were WNL.
Diagnosis: • Caleb suffers from the Fear of Aversive Consequences (or “Posttraumatic”) subtype of ARFID. • **Please note: This subtype of ARFID can be LIFE-THREATENING!**
Symptoms of Posttraumatic Feeding Disorder All Four Required: • Food refusal followed a major aversive event/noxious insult to oropharynx or GI tract. (Despite a hx of SFA in early toddlerhood, Caleb had been eating well for years. This sudden onset of food refusal followed a severe episode of GERD.) • He demonstrated a consistent refusal to eat – in his case it was eating of any solids (despite hunger and offering of preferred foods). It could also take the form of refusing all liquids or refusing both solids and liquids. • Any reminders of the traumatic event caused anticipatory distress and refusal to eat or swallow. (For Caleb, it was to the point that he could not even tolerate closing his mouth or swallowing his own saliva.) • Food refusal poses an acute or long-term threat to child’s nutrition. In Caleb’s case, he experienced risks that were both physical and emotional. • Lab abnormalities • Missing significant amount of school • Social isolated from his peers during food-related activities
Risk Factors for Posttraumatic Feeding D/O • Underlying separation anxiety • Choking, gagging, vomiting episodes • Medical instrumentation of the oropharynx • Insertion of nasogastric feeding tubes, endotracheal tubes, suctioning of oropharynx
Treatment of Posttraumatic Feeding D/O • Gradually introduce foods back into the child’s diet • Hierarchical fear food list • Treat the underlying anxiety with liquid SSRI, if needed. • Vitamin (liquid) supplementation may be necessary. • Consider use of enriched • Be mindful that patient is not filling up solely on supplements. • Offer food first and liquid supplements only afterward.
Case 3 • 16 yo female admitted for weight loss and vomiting over 1 week. • 10 pound weight loss over 6 days • Reports loss of appetite for past week • Fatigue • Hx of anxiety/panic attacks prior to onset of vomiting • Hx of presenting to the ED 2 weeks ago with chest pain
Case 3 • Afebrile • GI consult: Endoscopy and Abd USG wnl, ruled out SMA • Treated with antibiotics for presumed H. Pylori to explain vomiting, later test negative
Case 3 • Medications: • (Not tolerating any meds PO) • Amoxicillin 500 mg Q8h, • Clarithromycin 500 mg Q12h, • Alprazolam 0.5 mg Daily PRN for anxiety, • Zofran 4 mg Q8h PRN (ineffective)
Case 3 • Prior to onset of vomiting • Ate 3 meals a day with good hunger drive • No sensory sensitives to food • No restriction based on calories • No concerns for body image, feels good about how she looked prior to weight loss • Following onset of vomiting • Reported some initial hesitation to eat as she vomits every time she eats
Case 3: Diagnosis • ARFID based on • negative GI w/u • No organic cause for vomiting and some concern that anxiety may be triggering vomiting • Restrictive eating secondary to aversive reaction to vomiting
Case 3: Treatment • Placed on modified ED protocol • Given 3 meals a day based on 1800 kcal • Able to eat but unable to keep food down • Given NG tube and overnight feeding • Started Compazine • Able to gain weight during hospitalization (secondary to NG feeds)
Case 3: Admission 2 • Readmitted after 4 weeks • Attempting to eat small, multiple meals a day • Unable to keep food down • Lost 2 more kg • Still denying aversion to eating/food • New symptom: weakness and difficulty walking, attributed to malnutrition • Second GI consult: Nothing new • Still treated for ARFID and d/c
Case 3: Admission 3 • Readmitted after 3 weeks • Progressive B/L LE weakness • Progressive B/L LE numbness • Blurry vision: Optho visit unveiled left CN VI palsy • Outpt neuro: Sensory level ~T4, gait ataxia, b/l Babinski, clonus at both ankles
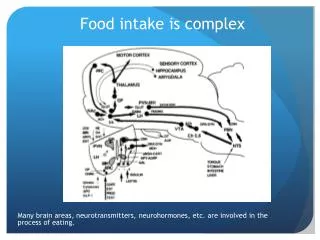
Case 3 • MRI brain/spine • Long-segment demyelinating disease with a lesion from the pons to the medulla and another from T4 to T10 • Vomiting = demyelinating lesion in medulla • Take home: ARFID diagnosis does not explain etiology