Download
1 / 57
640 likes | 928 Views
The role of IMSI in sperm selection. Monica Antinori. R.A.P. R.U.I International Associated Research Institute for Human Reproduction Rome , Italy. INTRODUCTION.

E N D
The role of IMSI in sperm selection Monica Antinori R.A.P.R.U.I International Associated Research Institute for Human Reproduction Rome, Italy.
INTRODUCTION A different prognosis can be assigned on the basis of different normal morphology thresholds (poor prognosis: ≤4%; good prognosis: 5-14%; normal: >14%) in order to choose an adequate infertility management . Kruger et al., 1988; Grow et al., 1994 Predictive value of sperm morphology for fertilization and pregnancy outcomes in IVF treatments. Kruger et al., 1986; 1987; Parinaud et al., 1993; Ombelet et al., 1997; Eilish T. et al., 1998 Correct selection of spermatozoa improves ICSI outcome Kahraman et al., 1999; Miller and Smith, 2001; De Vos et al., 2003
INTRODUCTION II According to some authors, ICSI outcome is not related to strict morphology of the sperm used for microinjection Oehningeret al.,1995; Kupker et al.,1998; Host et al.,2001; Celik-Ozenci et al.,2004 No differences in terms of fertilization and clinical pregnancy rates have been shown when samples with poor morphology (<5% normal cells) were used Gomez 2000 Fertilization, embryo development and pregnancy seem to be achievable even if normal spermatozoa are not available (100% of terato-zoospermia) Nagy et al., 1995; Tasdemir et al.,1997; Mckenzie et al., 2004
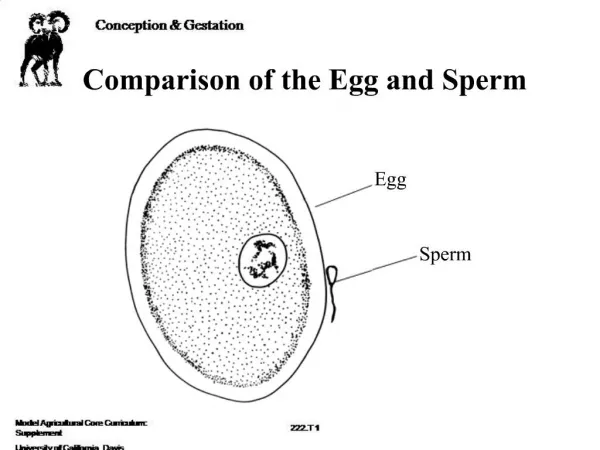
In the routine ICSI procedure, sperm cells are selected from the sperm pool under a regular microscope that magnifies 200-400x Recently new devices to achieve high magnification levels (6600x) have been proposed in order to detect subtle ultra-structural alterations that would be impossible to identify with conventional methods.
. Sperm sub-cellular organelles Bartoov , et al.,1999
Specific Morphological Malformations of the Sperm Cell Subcellular Organelles (other than nucleus) Observed by MSOME
ACROSOMAL LACK VACUOLES Bartoov , et al,1999
Criteria for morphologically normal nucleus -Oval shape -Longitudinal symmetry -Smooth content
Oval Shape LARGE OVAL Normal shape WIDE 4.75μm (±0.28) NORMAL SHORT LONG 3.28μm (±0.20) SMALL OVAL NARROW
Smooth Content No vacuoles/only one vacuole with a diameter greater than 0.78±0.18µm Vacuolated spermatozoa No extrusion or invagination of the nuclear chromatin mass Regional disorder I E
vacuoles estrusion
Sperm Functional Morphology is based on: • -High power light microscopy • -Single cell examination • -Real time observation • -Examination of only motile sperm cells • -Fine organellar morphology • MotileSpermOrganellar Morphology Examination MSOME
97 men from an unselected group of couples undergoing infertility investigation
Bartoov • Cassuto & Barak • Vanderzwalmen • Our proposal • Equipment • Chablon design
30 patients in an unselected group of couples undergoing infertility investigation and treatment Franco et al. 2008
Mitosensor Acridine orange Tunel Aneuploidies
Oliveira 2010 5- 50% vacuolized > 50% vacuolized
RBM Online2010 • Msome and acrosomal status assessment were simultaneously performed on 3237 spermatozoa of 30 man with the following sperm parameter: • concentration 65.6±0.2 x 106/ml • Progressive motility: 43± 18% • Vitality:79 ± 7.8% • Normal morphology (David’s criteria):29 ± 4.6%
MSOME on acrosome reacting spermatozoa A:Some protruding blebs are visible in the anterior part of the head D:In the following picture the corresponding area shows a “vacuole-like” image Kacem et al. 2010
“Thoughts on IMSI” Giampiero Palermo et al. In : "Biennial Review of Infertility, Volume 2" New York Inc. Springer-Verlag; June 2011
January 2006 - June 2007 • Study design: prospective randomized • Original Group: 446 couples • Inclusion criteria : 1) at least 2 previous diagnoses of severe • oligo-astheno-terato-zoospermia • 2) at least 3 years of primary infertility • 3) the woman being 35 or younger • 4) an undetected female factor • COH: GnRH Antagonist regimen(ganirelix acetate) + rFSH • OPU 35-36h after HCG • Transfer D3
CONCLUSION IMSI resulted in a significantly higher pregnancy rate than ICSI in all treated cases (P = 0.004) and notably in patients with ≥ 2 failures for whom the success rate increased by over 100% (P = 0.017), which confirms the data already published in the literature
Number of fertiized eggs Number of top quality embryos Setti et al. 2010
Number of gestational sacs Number of Pregnancies Setti et al. 2010
2011 Unselected infertile population
Bartoov’s retrieval hierarchy of morphologically evaluated "second best" sperm cells with minimally impaired nuclei.
Cassuto & Barak SCORE SYSTEM Score of spermatozoa: 2 Head + 3 Vacuole + Base CLASS I (4-6) = 6 POINTS CLASS II (1-3) = 2 POINTS CLASS III (0) = 0 POINTS
VANDERLZWALMEN CLASSIFICATION VANDERLZWALMEN 2008
IMSI at RAPRUI January 2005 and Dec 2010: 2082 IMSI cycles Mean age: 36.6 yrs Couples with >previous ICSI 2 failures 46.4% Mean n° failures/couple in this group 3.87
MSOME evaluation in daily IVF routine ADDITIONAL CRITICAL POINTS • Expensive equipment to reach the necessary magnification (microscope, camcorder, composite system of lenses) • Experienced embriologists (hard training) • Work in pairs cold be usefull to increase accuracy of the evaluation • Time consuming