Download
1 / 65
690 likes | 1.47k Views
Carbapenem -resistant Enterobacteriaceae (CRE) and the Imperative for Antimicrobial Stewardship. Christopher Trabue, M.D. September 13, 2013. Outline. Background and Epidemiology Clinical significance and public health implications

E N D
Carbapenem-resistant Enterobacteriaceae (CRE) and the Imperative for Antimicrobial Stewardship Christopher Trabue, M.D. September 13, 2013
Outline • Background and Epidemiology • Clinical significance and public health implications • Multipronged approach to controlling CRE in healthcare facilities • Antimicrobial stewardship • Our experience here
E. coli KlebsiellaEnterobacter VRE MRSA
Enterobacteriaciae and beta lactam antibiotics And the relationship therein
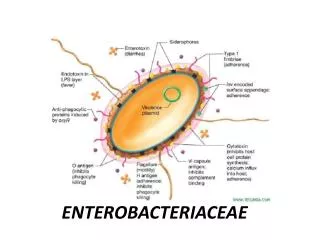
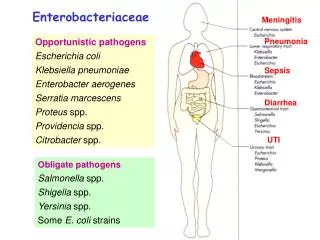
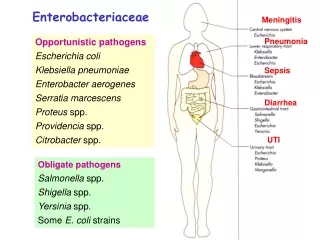
Enterobacteriaciae? • Enterobacteriaciae refers to a large family of gram negative bacilli that are commensal to the gastrointestinal tracts of mammals • Escherichia coli • Klebsiella species • Enterobacter species • Proteus species • Historically, these bacteria have been implicated in an array of human infection (UTI, nosocomial pneumonia, intra-abdominal infection) but have not been particularly associated with the epidemic of multidrug resistance until relatively recently
The clinical significance of beta lactam antibiotics • The beta lactam antibiotics comprise the penicillins, cephalosporins, carbapenems, and monobactams (aztreonam) • These agents easily comprise half of most hospital antibiotic formularies • Due to molecular innovations over the past 60 years, the antibiotic spectrum of these agents has been vastly expanded to cover a variety of different pathogens Penicillin Cephalosporin Carbapenem Aztreonam
Enterobacteriaciae – more and more beta lactamase • The primary mechanism of resistance for most enterobacteriaciae to beta lactam antibiotics is through enzymes known as beta lactamases • These are a heterogeneous group of enzymes in that hydrolyze (and thereby “open”) the beta lactam ring, inactivating it
CRE – an historical perspective Thalidomide
Obstetricians: No handwashing Midwives: Handwashing
Carbapenems – why they matter • Carbapenems are an essential component of the armamentarium against many gram negative pathogens and serve as a last line of defense • Pseudomonas aeruginosa • Acinetobacterbaumanii • ESBL-producing enterobacteriaciae • What about other agents with different mechanisms of action (ie, quinolones, aminoglycosides)? • Many plasmid genes that encode carbapenemases also encode resistance to other antimicrobials (ClinMicrobiol Rev. 2005 Apr;18(2):306-25) • In organisms with carbapenemases, resistance to other antimicrobials is highly probable
The Emergence of CRE The rise of the New Delhi metallo-β-lactamase and other CRE
NDM - Why India? • In India, there is little restriction on antibiotics which can be purchased cheaply without a prescription • Ciprofloxacin is a commonly used antibiotic in India • In India, pharmaceutical companies routinely discharge byproducts of pharmaceutical agents into sewage 30X MIC for many bacteria
CRE – increasing incidence • The incidence of CRE has increased sharply over the past decade • The point prevalence in two academic NY hospitals this year: 5.4% (Infect Control HospEpidemiol. 2013 Aug;34(8):809-17) TABLE 2. Number of Enterobacteriaceaeisolates reported — United States, National Nosocomial Infections Surveillance system, National Healthcare Safety Network CMAJ January 11, 2011 vol. 183 no. 1 59-64
CRE and mortality • As is the case with many resistant organisms, infections due to CRE are associated with significantly higher mortality • Numerous studies have placed mortality due to these infections in the 30-50% range Results: Case patients were more likely than control patients to die during hospitalization (48% vs 20%; P .001) and to die from infection (38% vs 12%; P .001). Setting: Mount Sinai Hospital, a 1,171-bed tertiary care teaching hospital in New York City. Design: Two matched case-control studies. 99 case patients, 99 controls. Infect Control HospEpidemiol 2008; 29:1099-1106
CRE – risk factors • Transplant recipients • Long term acute care hospitalization • 17.8% of LTACs reported at least 1 CRE-HAI versus 4.6% of acute-care hospitals in 2012 (MMWR Morb Mortal Wkly Rep 2013; 62: 165–70.) • Prior antibiotic therapy • Beta lactam antibiotics • Fluoroquinolones
CRE – treatment options • Treatment options are limited to say the least • Tigecycline • Novel glycylcycline antibiotic • Bacteriostatic, large volume of distribution (poor serum levels make it less than ideal for bacteremic infections) • Some data to suggest higher mortality in patients treated with this agent over beta lactam agents • Polymyxin B and E (Colistin) • Older agent (approved in 1958) • Potent, bacteriocidal activity • Significant toxicity (primarily nephrotoxicity in the 50% range) • There are numerous reports of CRE resistant to both agents
CRE and the challenge ahead There is hope….
CRE – Prevention Strategies • Hand Hygiene • Contact Precautions • Minimizing use of devices • Laboratory notification • CRE screening • Chlorhexidine bathing and intranasal mupirocin • Antimicrobial Stewardship 423 references!
Antimicrobial Stewardship Less is more….
What is ‘Antimicrobial Stewardship?’ • A process by which antimicrobial prescribing is optimized and improved based on available evidence and guidelines • Right agent/selection/combination/indication • Right dose • Right route • Right duration
Why? • In short, we are running out of antibiotics • Antimicrobial resistance is far outpacing research, development, and approval of new antibiotics • There is a lack of interest among pharmaceutical companies in developing new antimicrobial agents
And…. Not commercially available
What comprises a stewardship program? Administrative and Community Support
What does a stewardship program do? • Protocols and clinical pathways (ie CAP order set) • Dose optimization and therapeutic drug monitoring for vancomycin and aminoglycosides • IV to PO conversion • Active surveillance of hospital antibiotic use • Prospective audit, feedback, and education • De-escalation of therapy (ie, day 3 bundle) • Integration with infection control and clinical microbiology (ie, bug-drug mismatch) • Formulary restriction and preauthorization
Is there data supporting stewardship? • Yes. Lots. • On all fronts…. • Patient outcomes • Resistance • C-diff • LOS • Cost
Summary of rationale • Antimicrobial stewardship programs improve patient outcomes • Antimicrobial stewardship programs save money • Antimicrobial stewardship programs are ineffective without physician leadership and administrative support • We are in the process of developing and implementing an antimicrobial stewardship program (ASP) at Saint Thomas Midtown Hospital
ASP Pilot • In late 2012, with support from both URC and P&T, we were asked by MEC to conduct a pilot study examining antimicrobial stewardship at Saint Thomas Midtown Hospital • Principle investigators for this effort: Christopher Trabue, Ashley Tyler (clinical pharmacy specialist), Sharon Stacy (medical affairs) • The following criteria were developed for review: • Review of all patients with positive blood cultures on the IMSB service • Review of all patients on the IMSB service on ≥ 2 antibiotics for longer than 48 hours • Review of all patients on the IMSB service on antibiotics for longer than 7 days
ASP Pilot • Exclusion • ICU patients • IMSB consult patients • ID consult patients • During the study, all recommendations were communicated verbally to the attending physician if a change was recommended • De-escalation or escalation • Change • Discontinue • If a case was encountered where changes to therapy were considered which were too complex for our program, consultation was recommended
Metrics • Clostridium difficilerates • Mean use of IV antibiotics • Provider-specific antibiotic prescribing rates • Total antibiotic charges
Summary • Study Period: February 20, 2013 – May 17, 2013 • 172 patients met inclusion criteria for whom an intervention was indicated (297 total interventions)
Preliminary Results • Utilization rates for vancomycin, meropenem, IV and PO ciprofloxacin, IV levaquin, and ceftriaxone declined • Utilization rates for piperacillin-tazobactam (Zosyn) were essentially unchanged • Utilization rates for Levaquin PO increased • Improved cost associated with post-acute care (ie, more patients in Pilot group discharged home, rather than to SNF) • Still in process: • Clinical data – Sepsis/pneumonia/SSTI DRGs, attributable mortality, changes in Clostridium difficilerates • Provider-specific antibiotic prescribing rates • Total antibiotic charges