Download
1 / 14
140 likes | 152 Views
Explore the role of ACOs in improving care coordination, reducing costs, and enhancing patient outcomes within the evolving healthcare landscape. Learn how ACOs aim to address challenges like rising healthcare expenditures and fragmented care delivery. Discover the benefits of accountable care models and the impact on Medicare beneficiaries. Get insights into the goals and functions of ACOs under the Affordable Care Act.

E N D
Accountable Care Organizations (ACOs), Part 1 of 3 Migena Peno Pharm.D. Candidate LECOM School of Pharmacy
Background information • 1/5 patients readmitted within 30 days resulting in billions of $ every year in health care costs • Rising healthcare expenditures • Increase in patients >65 y/o & longer life expectancy • Multiple comorbidities • Rise in chronic conditions & higher obesity rates • Lack of access to health care (uninsured) • Lack of preventive care & early diagnosis • Emergence of new technologies • Labor costs S.F. Jencks, M.V. Williams, and E.A. Coleman. “ Rehospitalizations Among Patients in the Medicare Fee-for-Service Program,” New England Journal of Medicine. Apr 2, 2009. 360(14): 1418-28. Snapshots: Health Care Costs. Health Care Spending in the United States and OECD Countries. April 2011. National Center for Health Statistics. (2010). Deaths: Final Data for 2007. Hyattsville, MD. National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD.
Background information • Patients currently seeing multiple unrelated health care providers • Increased health care cost • Increased duplicate services • Lower quality of care • Payment not linked to performance • Lack of financial incentive to coordinated care • Physicians influence ~90% of health care spending • Fee-for-service does not promote lower-cost quality care Newman, D. Accountable Care Organizations and the Medicare Shared Savings Program. Congressional Research Service. Nov 4, 2010 Accountable Care Organizations: Improving Care Coordination for People with Medicare. HealthCare.
Background information • Current Medical system • Fragmented care among different providers • Pays for “units of service” not for outcome • No one is held accountable for quality on cost of care • Providers might be inclined to join ACO to: • Protect their place in market while preserving their autonomy • Share cost savings • Play a role in collective decisions Newman, D. Accountable Care Organizations and the Medicare Shared Savings Program. Congressional Research Service. Nov 4, 2010
What are ACOs? • “Organization of health care providers that agrees to be accountable for the quality, cost, & overall care of Medicare beneficiaries who are enrolled in the traditional fee-for-service program1” • “Healthcare organizations characterized by a payment and care delivery model that seeks to tie provider reimbursements to quality metrics and reductions in the total cost of care for an assigned population of patients2” Medicare” Accountable Care Organizations” Shared Savings Program – New Section 1899 of Title XVIII. Preliminary Questions and Answers. Center of Medicare and Medicaid Services. Accountable Care Organizations. American College of Osteopathic Family Physicians.
Affordable Care Act • Goals: • Keep health care costs low • Promote prevention • Hold insurance companies accountable • Fights Medicare fraud • Protects patients from abuse by insurance companies • Prevents higher premium charges or denial of policy due to pre-existing conditions FACT SHEET: The Affordable Care Act: Secure Health Coverage for the Middle Class. White House
Affordable Care Act • Limits the power of insurance companies to cancel policies • Includes policies to improve safety & quality of patient care & make care affordable • Main focus: Patients needs • Links payment to outcomes • Reduce health care costs while meeting performance standards on quality of care • Created “Medicare Shared Savings Program” to reward ACOs Accountable Care Organizations: Improving Care Coordination for People with Medicare. HealthCare. FACT SHEET: The Affordable Care Act: Secure Health Coverage for the Middle Class. White House.
CMS Innovation Center • Created by “Affordable Care Act” • Goals: Better health care, better health, & reduced costs for beneficiaries • Improvements in health care system • Identifying new ways to pay for & deliver care that improve care & health while lowering costs • Developing, supporting, & evaluating innovative models of payment & care service delivery for Medicare, Medicaid & CHIP beneficiaries Center for Medicare & Medicaid Innovation Center.
CMS Innovation Center • Better health care • Improving all aspects of patient care • Safety, Effectiveness, Patient-Centeredness, Timeliness, Efficiency, & Equity • Better health • Encouraging healthier lifestyles • Physical activity, good nutrition, avoiding behavioral risks, & using preventative care Center for Medicare & Medicaid Innovation Center.
CMS Innovation Center • Lower costs • Promoting preventative medicine • Improving coordination of health care services • Reducing waste & inefficiencies • Reduce national health care cost & out-of-pocket expenses for all Medicare, Medicaid, & CHIP beneficiaries Center for Medicare & Medicaid Innovation Center.
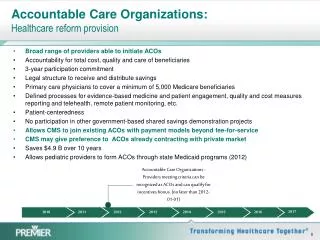
Accountable Care Organizations • A result of “Affordable Care Act” (March 2010) • Voluntary participation • Providing financial incentives for providing good quality care at low cost • Avoiding unnecessary tests & procedures • Save money + meet quality targets keep a portion of the savings • Fee-for-service payment system still used but bonuses provided if costs are kept down Gold J. Accountable Care Organizations, Explained. Kaiser Health News, NPR. Jan 18, 2011.
Accountable Care Organizations • Must share information within ACO • NOT a closed network or gatekeeper • Patients are not enrolled to ACO & have the freedom to choose their providers • Losing their bonuses, their contracts, & possibly paying a penalty if performance & savings benchmarks are not met • Providers in rural areas • Eligible to receive payments in advance to build the necessary infrastructure for coordinated care Gold J. Accountable Care Organizations, Explained. Kaiser Health News, NPR. Jan 18, 2011. In the private sector, the insured is still governed by the insurance contract between the insurer and the insured, and this contract may impose constraints such as differential coinsurance depending on whether an insured sees an in- network or out-of-network provider.
Accountable Care Organizations • Significant capital investment is required prior to earning any shared savings • Hospitals have the capability to provide the funds needed to start ACOs (staff, technology, & protocol costs) • Responsible for a “defined population of patients” insured by the payer & can not choose individual patients within that group based on their health status Newman, D. Accountable Care Organizations and the Medicare Shared Savings Program. Congressional Research Service. Nov 4, 2010 The more care the ACO is responsible for, the less likely the ACO is in the position to shift costs beyond its areas of responsibility. Hence, many ACO descriptions refer to the “entire continuum of care.”
Accountable Care Organizations • Upon contract, ACO & payer agree to a: • Benchmark (historic cost of care for the defined patient population) • Formula used to calculate anticipated changes in health care costs due to factors like increased medical care costs, aging, or changes in health care status • Targeted savings rate • Quality measures that must be met Newman, D. Accountable Care Organizations and the Medicare Shared Savings Program. Congressional Research Service. Nov 4, 2010