Download
1 / 45
470 likes | 830 Views
Encephalitis Brain Abscess. Reşat Özaras, MD, Prof. Infection Dept. A 37-year-old male Headache, stupor, tendency to sleep, fever, unaware to recognise the time and the place. Acute Encephalitis. The inflammation of the parenchyma of the brain especially that of the cerebral cortex.

E N D
EncephalitisBrain Abscess Reşat Özaras, MD, Prof. Infection Dept.
A 37-year-old male • Headache, stupor, tendency to sleep, fever, unaware to recognise the time and the place...
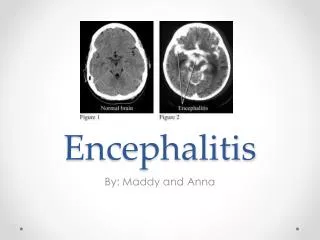
Acute Encephalitis • The inflammation of the parenchyma of the brain especially that of the cerebral cortex
The inflammation of the CNS • Encephalitis… the parenchyma...mostly due to viral infections • Meningitis… the meninges... mostly due to bacterial infections
Fever Headache Mental changes Confusion Hallucinations Personality changes Diplopia Fatigue Tremors Rash Loss of consciousness Symptoms
Acute Encephalitis • Mostly due to viral inf. • Herpes simplex virus (HSV) (the most common etiology of acute sporadic encephalitis) • Arboviruses – arthropod-borne virus (outbreaks in summer time…mosquitos and ticks) • Varicella zoster virus (VZV) (immunosuppressed patients)
HSV-1 • The most common etiology of acute sporadic encephalitis • HSV-1 • acquired in childhood period, • re-activates after years
Primary infection; On the mucosa of oropharynx, mostly asymptomatic fever, pain, dysphagia 2-3 weeks Following primary infection, a latent infection in trigeminal ganglion HSV-1
Inferior and medial temporal lobe Orbito-frontal lobe Limbic structures HSV-1 Inflammation necrotizing lesions Hemorrhagic necrosis in herpes encephalitis especially when remains untreated.
HSV-1 Widespreadedemaandsubarachnoidhemorrhageareas in medialtemporalandorbitofrontalregions
HSV-1 • Fever • Unilateral or generalized headache • Mental changes • Focal seizures • Focal neurological deficits • Dysphasia • Hemiparesis
VZV • Primary infection… chickenpox • Latent infection thereafter • The commonest reactivation… herpes labialis • Chickenpox, herpes labialis and zona may be complicated with encephalitis
Epstein Barr Virus • Causes infectious mononucleosis • May cause encephalitis • Direct invasion of CNS or immune mechanisms • Cortex, brain stem, basal ganglia, temporal lobe
CMV • Encephalitis in both immunocompetent and immunosuppressed • Risk is higher • immunosuppressed, • organ transplanted • HIV-infected patients • Organ transplantation, highest risk… CMV (-) donor to CMV (+) recipient
HIV • In 10-50% of AIDS patients, HIV infection in CNS • Multinuclear giant cells in gray matter and central white matter are pathognomonic.
Rabies • Lyssavirus • Acute progresive fatal encephalitis. • Transmitted with infected saliva of the animal • Incubation period: 5 days-6 mo.(20-60 days) • III, IV and IXth canial nerve palsies • Prodromal period, neurological disease period, paralysis, coma, and death.
Mumps • The commonest complication; inflammation in CNS • A pleocytosis in CSF in half of the cases • In 5-30%: headache, vomiting, neck stiffnes
History PE Neck stiffness CBC Biochemistry Culture Imaging Serology CSF analysis Clinical Evaluation
Season Localisation Travel Occupational exposure Exposure to animals Immunization Immune status of the patient History
Lab • CBC • Renal and hepatic tests • Coagulation studies • Plain chest X-ray Nonspecific Maindiagnosticmethods • CSF analysis • Cranial imaging
Cranial Imaging MRI Less sensitive than MRI CT • Sensitive for early period HSV encephalitis • Edema in orbitofrontal and temporal regions
Herpes simplex encepalitis CT(A) and MRI (B-F) temporal lobe involvement
CSF Analysis • Cell count: 10-2000 cells/mm3 • Mostly <500 cell/mm3 • Lymphocyte predominance • Erythrocytes (in 80% of the cases) • Normal CSF findings in 10% • Glucose (mg/dl): normal or low • CSF glucose/serum glucose: normal (>0.6) or low • Protein (mg/dl): >50 • Gram staining: no microorganisms • Culture: none
Microbiology • HSV PCR: For the first 24-48 hours, detecting HSV DNA by PCR in CSF: • specific (100%) and • sensitive (75-98%)
Herpes simplex encephalitis; Neurons including Cowdry A type intranuclear inclusion bodies. Hematoxylen-Eosin, X400.
Treatment • If shock/hypotension exists, crystaloid infusion • If unconscious, provide airway/breathing • Seizure, lorazepam 0.1 mg/kg, IV
Treatment • For encephalitis, give acyclovir
Treatment • Acyclovir IV, 14 – 21 days • HSV encephalitis • VZV encephalitis
Some keys • Atypical lymphocytes on peripheral smear… IMN • High amylase … Mumps
Complications Acute period Chronic period Chronic fatigue Depression Personality changes Gait disorders Memory disorders Speech disorders Visual problems Mental retardation Hemiplegia Seizure • Seizure • Inappropriate ADH synd. • Intracranial pressure inc. • Resp. arrest • Coma • Death
Prognosis • The virulence of the virus • Patient’s; • previous health status • immune status (chemotherapy, transplantation, AIDS) • age(<1, and >55 years) • any neurological symptoms
Prognosis • Being in coma on prsentation: severe inflammation in the brain, poor prognosis • Treated • Mortality… 20% • Morbidity… 40% • Untreated • Mortality … 50-75% • Morbidity… 100%
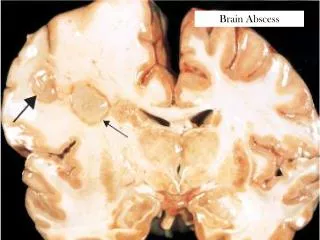
Brain Abscess • Focal collection in the brain parenchyma due to • Infection • Trauma • Surgery
Pathogenesis • Hematogenous: multiple abscess • Chronic pulmonary inf. (lung abscess, empyema…) • Skin inf. • Pelvic inf. • Intraabdominal inf. • Bacterial endocarditis • Cyanotic congenital heart dis.
Direct transmission • Subacute or chronic otitis media, mastoiditis (inferior temporal lobe and cerebellum) • Frontal or ethmoid sinusitis (frontal lobes) • Dental infections (frontal lobes)
Early lesion (first 1-2 weeks): • The borders are not clearly defined, localised edema • Inflammation, no necrosis • “Cerebritis” • After 2-3 weeks, necrosis • A fibrous capsule
Etiology • Aerobs+Anaerobs
Signs&Symptoms • Headache • Fever • Neck stiffness • Mental changes • Nausea, vomiting
Warning • LP is contraindicated!
Diagnosis • Imaging • MRI • CT
Treatment • Intervention • Antibiotics • Ceftriaxone + metronidazole Mortality 0-30 %