Download
1 / 67
720 likes | 950 Views
Treating Cancer with Charged Particles. Claire Timlin Particle Therapy Cancer Research Institute, Oxford Martin School, University of Oxford Slides are a PTCRi group effort. Contents. Introduction to Charged Particle Therapy Production and Delivery of Medical Proton Beams

E N D
Treating Cancer with Charged Particles Claire Timlin Particle Therapy Cancer Research Institute, Oxford Martin School, University of Oxford Slides are a PTCRi group effort.
Contents • Introduction to Charged Particle Therapy • Production and Delivery of Medical Proton Beams • Introduction to the Particle Therapy Cancer Research Institute • Research Projects • Malignant Induction Modelling • Virtual Phantoms • Data Recording and Sharing • Biological Effectiveness of Particle Beams • Clinical Ethics of Charged Particle Therapy • Proton Therapy in the UK PP Seminar
Introduction to Charged Particle Therapy PP Seminar
Development of Radiotherapy • 1895: Wilhelm Conrad Rontgen discovers X-rays • 1896: First x-ray treatment 3 months later! • 1898: The Curies discover radium • 1905: First Curie therapy • birth of brachytherapy PP Seminar
The Evolution of External Beam Radiation Therapy 1950’s The First Cobalt Therapy Unit and Clinac 2000’s? 1990’s Computerized 3D CT Treatment Planning 1980’s 1970’s Functional Imaging CerrobendBlocksElectron Therapy Multileaf Collimator Dynamic MLC and IMRT Standard Collimator High resolution IGRT Particle Therapy PP Seminar Slide courtesy of Prof. Gillies McKenna
History of Proton Therapy • 1946: • Therapy proposed by Robert R. Wilson, Harvard Physics • 1955: • 1st Proton Therapy at Lawrence Tobias University of California, Berkeley • 1955-73: • Single dose irradiation of benign CNS lesions • 2010: • > 67 000 patients had been treated with protons worldwide • 29 proton therapy centres operating worldwide • ~ 20 more planned or under construction Proton Therapy Centres Worldwide http://www.uhb.nhs.uk/ProtonsBirmingham/background/facilities.htm PP Seminar
Densely ionising radiation (high-LET) e.g. -particles C6+ ions High concentration of ionisation events Low vs. High Linear Energy Transfer Radiation Sparsely ionising radiation (low-LET) e.g. -rays, -particles Low concentration of ionisation events electron tracks DNA PP Seminar Slide courtesy of Dr Mark Hill
Radiation Induced Damage • Central Nervous System • blindness, deafness, paralysis, confusion, dementia, chronic tiredness • Bowel • colostomy, chronic bleeding. • Lung • shortness of breath • pneumonias • Kidney • renal failure and hypertension • Reproductive organs • sterility • Everywhere: • severe scarring in medium to high dose regions • possible increase in induced cancers in low-medium dose regions • Therefore must avoid dose to normal tissues.......... PP Seminar
Conformal Radiotherapy • Advantages • Reduced dose to organs at risk • Fewer complications • Increased tumour dose • Higher probability of tumour control • Disadvantages • Requires precise definition of target • Complicated planning and delivery therefore expensive! • Large volumes of low-intermediate dose (e.g. IMRT) -> secondary cancers PP Seminar
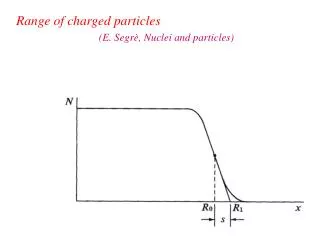
Photon vs. Proton/Ion Depth-dose Curve Photons Protons Dose Carbon Ions • High energy photons favoured over low energies due to skin sparing • Dose falls off but not to zero • Density of ionizations increase as the particles slow down -> peak in dose • No dose past peak Depth PP Seminar
The Spread Out Bragg Peak Unnecessary dose Skin sparing Unnecessary dose Incident energy is modulated to form spread out Bragg Peaks the cover the tumour PP Seminar
Combining Fields 80 50 150 0 60 150 0 40 X-Rays Protons/Ions PP Seminar
IMRT vs. Proton Therapy PP Seminar
Medulloblastoma in a Child X-rays 100 60 10 With Xrays With Protons PP Seminar
Orbital Rhabdomyosarcoma Protons/Ions X-Rays PP Seminar Courtesy T. Yock, N. Tarbell, J. Adams
Proton Therapy in ActionAnaplasticEpendymoma Brain Tumour http://news.bbc.co.uk:80/1/hi/england/7784003.stm 15th Dec http://news.bbc.co.uk/1/hi/england/7795909.stm 19th Dec http://news.bbc.co.uk/1/hi/england/7906084.stm 23rd Feb Pre-treatment During-treatment Post-treatment CPC, Friedmann, NEJM, 350:494, 2004 PP Seminar Slide courtesy of Prof. Gillies McKenna
HIT, Germany Beam Acceleration • Cyclotron • Protons up to ~250 MeV • Requires degraders • High current • Small(ish) • Simple(ish) • Main Manufacturers • IBA ,Varian • Best choice for protons at present? • Synchrotron • Carbon up to 400MeV/ • Dynamic energy change • Lower current • Bigger • More complicated • Main Manufacturers • Hitachi, Siemens • Only viable choice for heavy ion therapy at present? Future accelerators that do the job better? e.g FFAG, Laser Driven? PP Seminar
Beam Transport • Gantries • Fixed Beams • Clinical Indications • Flexibility • Space • Cost PP Seminar
Beam Delivery - Scanning • Parallel proton pencil beams are used (~3mm σ ) • Sweeper magnets scan the target volume in transverse plane (steps of 4mm) • One litre target volume typically 10000 spots are deposited in less than 5min. Beam direction Target Patient Beam direction Target Patient PP Seminar
Beam Delivery - Scattering Courtesy of T. Lomax, PSI, Switzerland. PP Seminar
Introduction to the Particle Therapy Cancer Research Institute PP Seminar
The Particle Therapy Cancer Research Institute PTCRi PP Seminar
The PTCRi Collaborators • Also work closely with (not an exhaustive list!): • Oxford Radcliffe Hospitals Trust • CERN • Mayo Clinic, Minnesota, USA • RAL • Ethox, University of Oxford • Maastro, Maastrict, Netherlands • Electa-CMS, Germany • For more info on the PTCRi team see: http://www.ptcri.ox.ac.uk/people/ PP Seminar
Challenges in Charged Particle Therapy Database for multiple parallel radiobiological calculations (with Jim Loken) -> sensitivity analyses Voxelised virtual phantom At treating centres New, improved radiobiological experiments on cells (and small animals)? Prostate study with Maastro FFAG (PAMELA), laser driven accelerators. EU Projects: ULICE, PARTNER, ENLIGHT. • Which particle (, p, C)? • Radiobiology • Cost-effectiveness • Which clinical indications? • Clinical ethics • Treatment Planning and Delivery • MC vs. treatment planning algorithms • Biological heterogeneity • Uncertainty in radiological models and parameters • Organ Motion • Recording and sharing clinical data • Late effects e.g. carcinogenesis • Accelerator design Investigating equipoise and clinical utility in collaboration with ETHOX. Oxford PT centre or collaboration? Radiobiological modelling validated with existing cell, small animal and clinical data Radiobiological modelling validated with existing cell, small animal and clinical data. PP Seminar
Novel Accelerator and Gantry Design PP Seminar
FFAG Accelerator • Fixed Field Alternating Gradient synchrotrons, FFAGs, combine some of the main advantages of both cyclotrons and synchrotrons: • Fixed magnetic field – like a cyclotron • fast cycling • high acceptance • high intensity • easy maintenance • high reliability • Strong focussing – like a synchrotron • beam extraction at any energy • higher energies or ion acceleration PP Seminar
FFAG Gantry A PAMELA NS-FFAG Gantry conceptual design Conventional Carbon Gantry at Heidelberg • Gantry is a beam delivery system which can rotate around the patient in 3600 • Delivering beams, avoiding critical organs and minimal transverse irradiation • Consists of bending magnets, focusing magnets, beam scanning system • Only one C- ion gantry existing at present , weighs ~600 tons • Use of FFAG technique is expected to reduce the size considerably PP Seminar
plasma sheath metal foil e- - - - + - - + - + - - + - Pulsed laser - ions + - - + + - - - + + - - + - - + - - Contaminant layer Laser Driven Ion Acceleration (Target Normal Sheath Acceleration-TNSA) • High intensity (>1019 Wcm-2) laser irradiate thin foil (~10μm) • Laser electric field is higher than atomic electron binding energy (~1016 Wcm-2) and the surface will be instantly ionised and plasma is created. • Laser electric field and magnetic field drive plasma electrons into the target with relativistic energies • Some of the energetic electrons escapes through the rear side of the target (non irradiated surface) and large space charge is generated on the rear surface. • This sheath field is of the order of ~1012 Vm-1, ionises rear surface and accelerate ions to MeV energies (generally present in the form of contaminants) • Any ion species can be accelerated PP Seminar
Advantages and Challenges of Laser Driven Ion Acceleration Advantages • Extremelaminarity: rmsemittance< 0.002 mm-mrad • Short duration source: ~ 1 ps • High brightness: 1011 –1013 protons/ions in a single shot (> 3 MeV) • High current : kA range • minimal shielding and expensivemagnets are not required Challenges • Clinicalenergies are not achievedyet (~65MeV proton atpresent) • Energyspread, repetition rate, neutron contamination, beamstability… PP Seminar
Malignant Induction Modelling PP Seminar
Mis-repair Mutation Transformation Radiation Action on Cells Direct DNA damage DNA dsb Repair No repair Cell survival Cell death PP Seminar Slide courtesy of Prof. Boris Vojnovic
Induction and cell kill Form of cell killing function known with some certainty at clinical energies, the parameters are tissue dependent and can have large uncertainties. What is the form of the induction function? Linear, quadratic? Cell killing Induction Probability the cell survives Probability of transforming a cell • Risk needs to be • accurately modelled • confirmed experimentally • taken into account when deciding on the optimal treatment plan Probability of inducing a potentially malignant mutation PP Seminar
Voxelised 3D Calculations of Biological Endpoints • Model and parameter sensitivity analyses • Validation with clinical data on secondary malignancies PP Seminar
Virtual Phantoms PP Seminar
Virtual Phantoms • Virtual phantom provides an anthropomorphic reference geometry for Monte Carlo particle transport • Two flavours: • Nowadays have the memory and processing power to deal with megavoxels Computationally intensive voxellised phantoms (3D equivalent of pixels) Geometrically simple mathematical phantoms (cylinders, spheres, cones, etc...) PP Seminar
Virtual Phantoms • ICRP Reference Man consists of 7 million voxels (3D pixels) • Each voxel assigned an organ type that specifies density, elemental composition, etc. • Size and masses typical of average man • Female phantoms also exist, children being developed PP Seminar
PTCRi Phantom work • ICRP man has been converted to a simulated CT scan • can be input into treatment planning software • Enables assessment of TPS accuracy by comparison to Monte Carlo: • Accuracy of the TPS method of mapping CT number (x-ray linear attenuation coefficient) to proton stopping power • Effect of air cavities and tissue boundaries on the range and profile of proton beams • Also interested in examining the second cancer induction risk due to scatter from the beam head. PP Seminar
Data Recording and Sharing PP Seminar
EU Projects: ENLIGHT and PARTNER http://enlight.web.cern.ch http://partner.web.cern.ch PP Seminar Slide courtesy of Faustin Roman 40
EU Project: ULICE • ULICE: Union of Light Ion Centres in Europe • Aims: • Transnational access to particle radiotherapy facilities • Facilitating joined up research across Europe • Addressing efficacy and cost-benefits for CPT • Methods: • developing and recommending standards for key observations and measurements in CPT • facilitate data sharing and reuse through pan-European collaborative groups • at the point at which key European centres are commissioning facilities PP Seminar
European Heavy Ion Centres Centres in Europe treating with heavy ions NRoCK (Kiel) RKA (Marburg) Connect centres ... ... and make most of available data! MedAustron (Wiener Neustadt) HIT (Heidelberg) CNAO (Pavia) ETOILE (Lyon) PP Seminar
Data Sharing and Interpretation - Challenges Medical Doctor Statistician Platform for translational research and clinical practise (1/2) data owners Users clinicians from multiple disciplines with specific views on data researchers Biologist across Europe Chemist with different levels of technical knowledge Physicists with different privileges Data Common access point from multiple disciplines with specific terminologes stored across Europe CONFIDENTIAL In various independent repositories CONFIDENTIAL with different ethical and legal requirements PP Seminar
GRID? : Coordinated resource sharing and problem solving in dynamic, multi-institutional virtual organizations… (I. Foster et al) HadrontherapyInformation Sharing Platform (HISP) Prototype connecting: • Users • Data sources with • Grid resources • Security framework • Data integration services by • Portals • Interfaces USECASES: 1. REFERRAL 2.RESEARCH PP Seminar Slide courtesy of Faustin Roman
A patient opinion… http://www.nature.com/nm/journal/v16/n7/full/nm0710-744.html PP Seminar Slide courtesy of Faustin Roman
Biological Effectiveness of Particle Beams PP Seminar
Relative Biological Effectiveness • Photons and protons (at clinical energies) have similar biological effects • Clinically a modifier (RBE) of 1.1 is applied to physical dose for protons • For heavier ions (e.g. C) RBE has large uncertainties • RBE needed* to calculate physical dose to administer to achieve prescribed biological dose *maybe there is a better way? New treatment regimes requiring new methods of optimisation? PP Seminar
RBE vs. Dose for Protons Where does the 1.1 come from? Paganettiet al.: Int. J. Radiat. Oncol. Biol. Phys. 2002; 53, 407 PP Seminar
RBE vs. Dose for Protons More data is required to determine magnitude of proton RBE variation with dose for a variety of tissues Where? CERN? V79 Cells. Wouterset al.:Radiat Res 1996 vol. 146 (2) pp. 159-70 PP Seminar
Modeling RBE vs. Dose for Carbon RBE increases with decreasing dose Analysis of 77keV Data from Suzuki et al, IJRBP, Vol. 48, No. 1, pp. 241–250, 2000 PP Seminar