Download
1 / 19
190 likes | 324 Views
When you feel fatigue and it seems as if you are less energetic then it is high time to get your Thyroid checked. It might be Hypothyroidism, a very common phrase we hear these days affecting people in an enormous way. This is a condition where certain functions of the body is measured down leading to fatigue and various other problems.

E N D
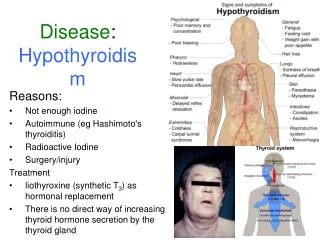
INTRODUCTION • Hypothyroidism is defined as a deficiency in thyroid hormone secretion and action that produces a variety of clinical signs and symptoms of Hypometabolism. • Overt Hypothyroidism is defined as an elevated serum TSH concentration (usually above 10 mIU/L) and reduced free Thyroxine concentration (fT4) • Subclinical Hypothyroidism is defined as serum TSH above the upper reference limit in combination with a normal free Thyroxine (fT4)
Prevalence • According to a projection from various studies on Thyroid disease, it has been estimated that about 42 million people in India suffer from Thyroid diseases. The prevalence of Hypothyroidism was 3.9%. The prevalence of subclinical Hypothyroidism was 9.4%. In women, the prevalence was higher, at 11.4%, when compared with men, in whom the prevalence was 6.2%. The prevalence of subclinical Hypothyroidism increased with age. About 53% of subjects with subclinical hypothyroidism were positive for anti-TPO antibodies.
CLINICAL PRESENTATION • Hypothyroidism can affect all organ systems & these manifestations are largely independent of the underlying disorder but are a function of the degree of hormone deficiency.
HASHIMOTO’S THYROIDITIS • Hashimoto’s Thyroiditis is an autoimmune disease in which the thyroid gland is attacked by a variety of cell and antibody-mediated immune processes, causing primary Hypothyroidism. The resulting inflammation from Hashimoto’s disease, also known as Chronic Lymphocytic Thyroiditis, often leads to an underactive Thyroid gland (Hypothyroidism). • The diagnosis of Hashimoto’s Thyroiditis is supported by recognition of autoantibodies against TPO or Thyroglobulin. 90% of patients with Hashimoto’s Thyroiditis have anti-TPO antibodies and anti-Thyroglobulin antibodies, making these antibodies excellent markers for Hashimoto’s Thyroiditis. Anti-TPO antibody positivity is more common at the time of diagnosis than anti-Thyroglobulin antibody.
Hypothyroidism in Pregnancy • Convincing data suggest that pregnant women who are positive for Thyroid autoantibodies (especially anti-TPO antibodies) leads to higher frequency of miscarriage (13.8%) than is seen in pregnant women who lack anti-TPO antibodies (2.4%), and that T4 treatment of the anti-TPO antibody positive group reduces the risk of miscarriage to approximately 3.5%. • Over Hypothyroidism (OH) in pregnancy is defined as an elevated TSH (>2.5 mIU/L) in conjunction with a decreased FT4 concentration. Women with TSH levels of 10.0 mIU/L or above, irrespective of their FT4 levels, are also considered to have OH. • Sub-clinical Hypothyroidism (SCH) in pregnancy is defined as a serum TSH between 2.5 and 10 mIU/L with a normal FT4 concentration. • Isolated Hypothyroxinemia (IH) is defined as a normal maternal TSH concentration in conjunction with FT4 concentrations in the lower 5th or 10th percentile of the reference range.
Prevalence • 10%-20% of all pregnant women in the first trimester of pregnancy are Thyroid Peroxidase (TPO) or Thyroglobulin (Tg) antibody positive and Euthyroid • 16% of the women who are Euthyroid and positive for TPO or Tg antibody in the first trimester will develop a TSH that exceeds 4.0 mIU/L by the third trimester, and 33%-50% of women who are positive for TPO or Tg antibody in the first trimester will develop postpartum Thyroiditis • 2%–3% of apparently healthy, non-pregnant women of childbearing age have an elevated serum TSH. Among these healthy non-pregnant women of childbearing age it is estimated that 0.3%-0.5% of them would, after having Thyroid function tests, be classified as having OH, while 2%–2.5% of them would be classified as having SCH
Specific adverse outcomes associated with maternal Hypothyroidism include: • An increased risk of premature birth, low birth weight, and miscarriage. Such patients carry an estimated 60% risk of fetal loss when OH was not adequately detected and treated • Negro and colleagues published data suggesting SCH also increases the risk of pregnancy complications in anti-thyroid peroxidase antibody positive (TPOAb+) women • Negro et al. reported a significantly higher miscarriage rate in TPOAb+_ women with TSH levels between 2.5 and 5.0 mIU/ L compared with those with TSH levels below 2.5 mIU/L
Recommendations: • Women who are positive for TPOAb and have SCH should be treated with LT4 • Women with SCH in pregnancy, who are not initially treated, should be monitored for progression to OH with a serum TSH and FT4 approximately every 4 weeks until 16-20 weeks gestation and at least once between 26 and 32 weeks gestation • Isolated Hypothyroxinemia should not be treated in pregnancy
Recommendations: • Anti-Thyroid Peroxidase Antibody (TPOAb) measurements should be considered when evaluating patients with subclinical Hypothyroidism. • If anti-thyroid antibodies are positive, Hypothyroidism occurs at a rate of 4.3% per year versus 2.6% per year when anti-thyroid antibodies are negative. • Assessment of serum free T4, in addition to TSH, should be considered when monitoring L-thyroxine therapy. • Treatment based on individual factors for patients with TSH levels between the upper limit of a given laboratory’s reference range and 10 mIU/L should be considered particularly if patients have symptoms suggestive of Hypothyroidism, positive TPOAb or evidence of atherosclerotic cardiovascular disease, heart failure, or associated risk factors for these diseases.
Recommendations: • Patients whose serum TSH levels exceed 10 mIU/L are at increased risk for heart failure and cardiovascular mortality, and should be considered for treatment with L-thyroxine. • Euthyroid women (not receiving LT4) who are TPOAb + require monitoring for Hypothyroidism during pregnancy. In addition to the risk of Hypothyroidism, it has been described that being TAb + constitutes a risk factor for miscarriage, premature delivery, Perinatal death , post-partum dysfunction, and low motor and intellectual development (IQ) in the offspring.
References: • Indian Journal of Endocrinology & Metabolism. 2011 Jul; 15(Suppl2): S78–S81. • Williams text book of Endocrinology, Eleventh edition • Tietz Textbook of Clinical Biochemistry, Fifth Edition • Clinical Practice Guidelines for Hypothyroidism in Adults: Cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association
References: • Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A 2010 Universal screening versus case finding for detection and treatment of thyroid hormonal dysfunction during pregnancy. J ClinEndocrinolMetab 95:1699–1707. • Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A 2010 Increased pregnancy loss rate in thyroid antibody negative women with TSH levels between 2.5 and 5.0 in the first trimester of pregnancy. J ClinEndocrinolMetab95:E44–8
For more information about Health Disease visit https://www.lalpathlabs.com Hyperthyroidism