Download
1 / 29
290 likes | 396 Views
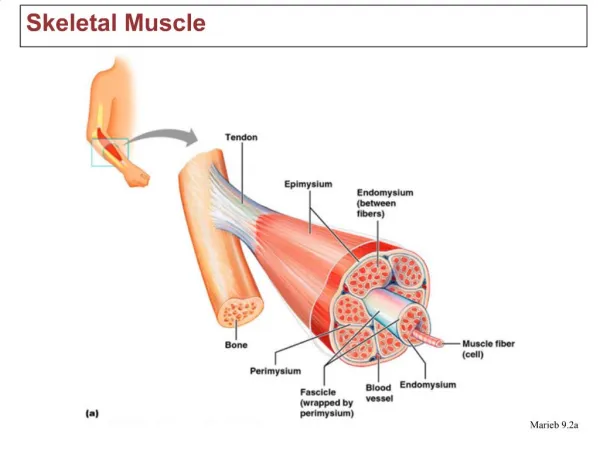
Electron Micrograph of RyR1 Ryanodine Receptor in Skeletal Muscle. “Catecholamine Induced RyR1 Ca 2+ Release in Malignant Hyperthermia Sensitive Human B-Lymphocytes. Lt. Colonel Susan M. Perry, PhD, CRNA, USAF, NC. Disclaimer.

E N D
Electron Micrograph of RyR1 Ryanodine Receptor in Skeletal Muscle “Catecholamine Induced RyR1 Ca2+ Release in Malignant Hyperthermia Sensitive Human B-Lymphocytes. Lt. Colonel Susan M. Perry, PhD, CRNA, USAF, NC
Disclaimer • The view expressed in this presentation are those of the authors and do not reflect the official policy or position of the Department of the Air Force, the Department of Defense, or the Uniformed Services University, or the United States Government. • Funding for this research was provided by a grant from the American Association of Nurse Anesthetist Foundation
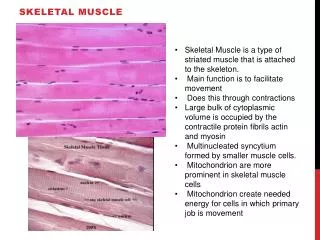
BACKGROUND • Malignant Hyperthermia (MH) is an autosomal inherited disorder associated with the RyR1 (Ryanodine) receptor in skeletal muscle that pre-disposes the susceptible individual to a life threatening hypermetabolic syndrome. Although it is predominantly exhibited during general anesthesia, exertional heat and emotional stress also have been shown to trigger MH. • Without the definitive treatment of dantrolene sodium and discontinuation of all triggering agents, mortality is in excess of 70%.
Graphic Representation: Clinical Signs of MH Ca2+ Release Melzer & Dietz Acta Physiol Scan, 2001
Unresolved Issues..what else acts as trigger? • MH in the absence of anesthetic triggers • 2 year old girl • Family History of MH • Machine was “clean” flushed overnight/10L/min • No triggering agent used/IV Propofol and morphine/glycopyrolate • Triggered 15 minutes into case • 57% NAMH/More than 2 uneventful anesthetics • Larach et al. 2010
MH and Stress in Humans • In the 1970s and 1980s there were many studies and case reports implicating emotional and exercise induced stress or pain as contributing to the development of MH in humans. • Moulds, 1975; Katz, et al. 1976; Huckell, et al., 1978; Gronert, et al., 1980; Wingard, 1981; Grinberg, 1983; Britt, et al., 1988; Montegi, et al., 1996; Muldoon, et al., 2004).
These questions continue today • Researchers Muldoon, Deuster, Brandom and Bunger examined the relationship between MH and exertional heat stress. In their paper they discuss variability as a “striking characteristic” of the disease MH. • These researchers suggested that MH “stems from an interaction between genes and environmental factors” and estimated that between “5-8%” of MHS individuals develop symptoms with exercise, emotional stress and or environmental heat exposure. • “Is There a Link Between Malignant Hyperthermia and Exertional Heat Injury?” Exercise and Sports Science reviews, 2004
Research Question • Is the variability seen in MHS individuals related to an abnormal adrenergic response related to an increased sensitivity to catecholamines? • I needed a human model.
Human Lymphocyte Model • Human B Cells express RyR1 • Sei, et al. (1999): • RYR1 expressed in human B-lymphocyte cell lines was identical to the skeletal muscle type (RYR1). • Ca2+ release in B cells was significantly altered by 4-chloro-m-cresol and ryanodine (J Biol Chem, 1999) • The Ca2+ responses to caffeine or 4-chloro-m-cresol in B lymphocytes showed significant differences between MHS and MHN (or control) individuals.(Anesthesiology,2002)
Human Lymphocyte Model • McKinney, et al. (2006): RyR1-mediated Ca2+ signals could be distinguished from other intracellular sources of Ca2+ in human B cells using fluorescent measurements of the response to the RyR1 agonist 4-chloro-m-cresol (4-CmC). • Lymphocytes from MHS pigs displayed increased sensitivity to 4-CmC when compared to cells from normal pigs. • (EC(50) = 0.47 vs. 0.81 mm for normal cells) • (Anesthesiology, 2006)
Hypothesis • Activation of the adrenergic stress response in malignant hyperthermia susceptible (MHS) B-lymphocytes will result in an augmentation of intra-cellular Ca2+ release in response to the RyR1 agonist 4 Chloro-m-cresol (4-CmC) in a way that is different from MHN cells.
Norepinephrine Protocol 50 Seconds 250 Seconds 0 1 2 3 4 0 = Cells at room temperature/ 40 minutes minimum 1 = Cells spun/ Fresh Buffer added/ Cells re-suspended 2 =Norepinephrine 1μM added to Cells 3 = Baseline measurement taken (50 seconds) and 4 CmC added to cells 4 = Area Under Curve measurement taken at 250 seconds/ Peak Fura 2 Emissions noted
4-CmC Dose Response in MHN Cell Line Yellow: 4-CmC alone Red: 4 CmC with NE
4-CmC Dose Response in MHS Cell Line Yellow: 4-CmC alone Red: 4-CmC with NE
Norepinephrine 4-CmC Response Results • MHS vs MHN groups demonstrated statistically significant differences in response to norepinephrine augmentation of 4-CmC Ca2+ emissions when comparing Base Area (BA), Peak Emissions (PE) and Area Under Curve (AUC). • P < .05 • Effect Size = 0.96
MHS vs MHN Baseline Area Ca 2+Emissions • Differences in Baseline Ca2+ emissions in the presence of Norepinephrine • MHS = 65 • MHN = 61 • P < 0.05 • Baseline responses were removed from analysis of 4-CmC response during analysis.
AUC Comparison for Fura 2 Ca2+ Emissions in MHS vs MHN Human B. Lymphocytes • There was no statistically significant difference in MHN AUC response to 4-CmC in the presence or absence of norepinephrine (P > .05). • There was a statistically significant difference in MHS cell lines response to 4-CmC in the presence of norepinephrine (P < .05). • There was a statistically significant difference in MHS vs MHN B-cell lines in AUC response to 4-CmC both in the absence and presence of norepinephrine (P < .05). • This was true for all doses of 4 CmC (paired student t-tests) • * 2.0m M Response may be non-specific for RyR1 Calcium Release alone AUC ANOVA Results
Fura 2 Ca2+ PE Comparison between MHS vs MHN Human B- Lymphocytes • There was no statistically significant difference in MHN PE Ca2+ response to 4-CmC in the presence or absence of norepinephrine (P > .05). There was a statistically significant difference in MHS cell lines PE Ca2+ response to 4-CmC in the presence of norepinephrine (P < .05). There was a statistically significant difference in MHS vs MHN B-cell lines in PE response to 4-CmC both in the absence and presence of norepinephrine (P < .05). This was true for all doses of 4 CmC (paired student t-tests) * 2.0 Response may be non-specific for RyR1 Calcium Release alone PE ANOVA Results
Norepinephrine/Propranolol Study Yellow: 4 CmC alone Red: 4 CmC with NE Teal: Propranolol Effect 4 Separate MHS Cell lines
Norepinephrine/Phentolamine Study Yellow: 4- CmC Alone Red: 4- CmC with NE Teal: Phentolamine Effect 4 Separate MHS Cell Lines
Isoproterenol/Propranolol Study Yellow: 4- CmC alone Red: 4-CmC with Isoproterenol Teal: Propranolol Effect 4 MHS Separate Cell Lines
Conclusions • Human B-Lymphocytes from Malignant Hyperthermia susceptible (MHS) individuals display a significantly increased sensitivity to norepinephrine induced adrenergic augmentation of intra-cellular Ca2+ release from the Ryanodine (RyR1) receptor when compared to MHN controls and this response is effectively blocked by the αadrenergic blocker phentolamine.
Conclusions • EBV Immortalized human B-lymphocytes provided a useful cell line model to examine intracellular Ca2+ handling under various hormonal and pathological conditions.
Conclusions • Because the Ca2+ release response was enhanced in the presence of a CONSTANT concentration of 1μM of norepinephrine, the data suggest that the MHS cell lines exhibit an increased sensitivity to adrenergic αagonists, compared to MHN cell lines.
Conclusions • The statistical evidence shows that only about 65% of the variability in the measured Ca2+ response in both the MHN and MHS cell lines can be attributed to RyR1 agonism due to 4-CmC in combination with norepinephrine. This means that 35% of the observed variability remains unexplained. I conclude from this that there should be other cellular mediators that contribute to the response. • The β adrenergic response requires further study.
Future Research • In Vivo study • Immune response in MHS and EHI individuals • Use in development of new testing/diagnosis in MH and EHI individuals
Future Studies and Limitations • Variability in numbers of adrenergic receptors on MHS B-Lymphocytes. • Intracellular stores of Calcium (Not only RyR1) • Immune cells vs myofibrils: What effect does stress have on immune response in muscle and immunology. • Limitations Immune cells vs myofibrils: need to examine effect on myofibrils.
Acknowledgements • Christine Kasper, PhD, RN, FAAN, FACSM, Professor, PhD Program, GSN, USU • Sheila Muldoon, M.D. Professor of Anesthesiology/Director of MH Diagnostic Center, USU • Rolf Bunger, M.D., PhD, Professor of Physiology, School Of Medicine, USU • Colonel Michaela Shafer, PhD, RN, Chief Nurse Executive, Assistant Professor, GSN, USU