Download

1 / 87
971 likes | 1.54k Views
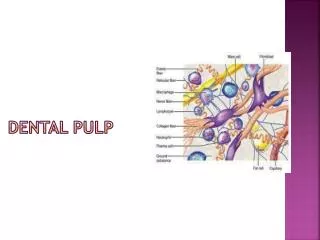
Pulp response to. preparation. cavity. Restorative materials. CONTENTS. Introduction Pathophysiology of pulpal infection Pulpal reactions Causes of possible pathologic response of pulp to operative procedures Reaction to operative procedures. Factors causing pulpal reaction

E N D
Pulp response to preparation cavity Restorative materials
CONTENTS • Introduction • Pathophysiology of pulpal infection • Pulpal reactions • Causes of possible pathologic response of pulp to operative procedures • Reaction to operative procedures
Factors causing pulpal reaction • Dessication of dentin • Vibratory phenomenon • Depth of cavity preparation • Speed of rotation • Heat and pressure • Dry cavity procedures
Nature of cutting instrument • Size of wheels and burs • Extensiveness of preparation • Pin restoration • Rebound response • Polishing of restoration
Chemical irritants • Dentin sterilizing agents • Cleansing and drying medicaments • Acid etchants • Bleaching Laser
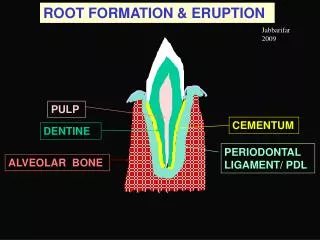
INTRODUCTION • The effect of restorative procedures on dentin and pulp represent a combined response to preparation and to restoration. • Every aspect of restorative dentistry potentially has an effect on pulp dentin complex.
Most of these effects are indirect, mediated via diffusion through dentin. • No restorative material exists that is truly inert in biologic sense and any Pulpal and dentinal change that result from the preparation can effect the evaluation of reactions to the entire restorative procedure.
Long term maintenance of a healthy pulp is a result of atraumatic preparationand the use of biologically acceptable materials that can seal the tooth restoration interfaceto prevent or minimize bacterial leakage.
Pulpal reactionsLangeland 1957,Stanley 1968 SLIGHT MODERATE SEVERE
Slight • in no of cells in cell free zone • fibroblasts & undifferentiated mesenchymal cells • Few inflammatory cells • Increase no of capillaries • Localized to affected dentinal tubules
Moderate reaction • More cells in area subjacent to affected dentin • Neutrophilic and mononuclear leukocytes invade odontoblast- predentin area • Increased number of capillaries & vessels are found in infiltrated tissue and its border
Severe reactions • Marked cellular infiltration with abscess formation • PMN’s & mononuclear leucocytes predominate in affected area • Odontoblastic layer cannot be identified • No predentin is formed and with in days existing predentin mineralizes
Causes of possible pathological responses of dental pulp related to operative dentistry
Physical: occlusal interference, condensation, air blowing or dentin dehydration • Thermal: heat from cutting, insufficient pulpal protection for metallic restoration • Electrochemical: galvanism • Chemical: toxicity of dental materials, acid etching
Bacterial: toxin products • Traumatic stimuli: abrasion, attrition, erosion dentin exposed • Operator: poor contour-contact, overhanged margin, poor anatomy, damage of adjacent tooth
Natural defense mechanisms • Dentinal sclerosis • Reparative dentin formation • Smear layer; controversial
Reparative dentin is a tertiary dentin matrix formed by new odontoblast like cells in response to a specific stimulus, while Reactionary dentin is formed by surviving odontoblasts subjacent to diseased or otherwise damaged dentin.
Reparative dentin under restorations • Avg. daily reparative dentin reported to be 2.8microns for deciduous and 1.5 microns for permanent teeth (stanley) • Begins earlier in shallow cavities • rate is more rapid but the quality is poorer than dentin formed under shallow preparation.
Restorative factors contributing to Pulpal injury Marginal leakage Cuspal flexure
Factors that might cause pulpal reaction Frictional HEAT Cleansing & Sterilizatn Vibration Acid etching Dessication Impressions Restorative materials Insertion & Cementation Marginal leakage of restorations Pulpal inflammation Pulpal NECROSIS. Probably [ Cohen ]
THERMAL INJURY PULP Goodacre’s conclusion • Thermal elevation low speed ˂ high speed ˂ ultrahigh speed. Goodacre quoted note of Ottl & Lauer : Thermal change : Carbide burs ˂ Diamond points. Temp ↑ : Fine diamonds ˂ Coarse diamonds.
THERMAL INJURY PULP Zach & Cohen : • An intrapulpal temp rise of 5.5°C (10°F) – 15% pulps become nonvital. (rate of heat application is more) • Recommended “WASHED – FIELD” Tech : Before cutting , tooth surface is exposed to the air-water spray for 5 sec. After initial cutting; following every 4 sec’s of cutting, bur is lifted off the surface for 1 second. (pulpal temp never rises above basal temp).
THERMAL INJURY PULP BLUSHING of teeth→ frictional heat. • Coronal dentin develops a pinkish hue {vascular stasis in the sub-odontoblasticcapillary plexus} very soon after the dentin is cut. • Under favourable conditions, this reaction is reversible & pulp will survive. • But dark purplish color → thrombosis → poorer prognosis.
Histologically →adjacent to blushed dentinal surface RBC’s extravasated (rupture of capillaries in sub-odontoblastic plexus). • Greatest beneath full-crown prepn
Crown Preparation In long term study on pulp vitality PULP NECROSIS • Full- crown preparation → 13.3 % • Partial veneer restorations → 5.1 % • Unrestored control teeth → 0.5 % • Foundations for full- crown restorations → 17.7 %
Desiccation of Dentin • Surface of freshly cut dentin → dried (while cutting or) with a jet of air → rapid outward movt of fluid thr’ dentinal tubules ( capillary action ). • Stimulatnof sensory nerves of pulp [ Acc to hydrodynamic theory ]. • Fluid movt also draw odontoblasts up into the tubules. • These displaced odontoblasts soon die (autolysis) & disappear. • But does not injure the pulp.
Ultimately, ODONTOBLASTS THAT HAVE BEEN DESTROYED AS A RESULT OF DESICCATN ARE REPLACED BY NEW ODONTOBLASTS THAT ARISE FROM THE CELL-RICH ZONE OF PULP & REPARATIVE DENTIN FORMS IN 1 to 3 MONTHS.
Vibratory Phenomenon • Shock waves produced by vibration are particularly pronounced when the cutting speed was reduced. • Therefore “STALLING OF THE BUR BY INCREASED DIGITAL PRESSURE ON THE HANDPIECE SHOULD BE AVOIDED”.
Increase the depth of preparation → Increased rate of reparative dentin formation. Only if RDT [bet pulp & base of cavity] half the original thickness Maximum threshold of stimulus will be reached. DEPTH OF PREPARATION & REPARATIVE DENTIN FORMATION
If further cutting Greater injury to odontoblasts Rate of formation of reparative dentindecreases { irregular structure, Poorly mineralized }. Even less thickness of dentin if remains- formation of reparative dentin inhibited temporarily & Odontoblastic cells show signs of atrophy.
Kinetic Cavity Prepn=Airborne Particle Prepn = Microprepn • Due to advances in microabration technology • Precisely remove enamel & dentin. • Laurell et all found that higher pressures & small particles had significantly fewer pulpal effects than the high- speed treated teeth. • stream of particles cannot be controlled, resulting in pitting & abratn of adjacent teeth & injury to gingival tissues.
Depth Of Cavity Preparations Cavity preparation causes • Increased rate of collagen turn over • Odontoblastic cell damage • Protein synthesis by odontoblasts directly under and adjacent, to the cavity prep is curtailed. • As cavity depth if increased more severe is injury to odontoblasts – increase rate of production of rep dentin.
With 0.5mm of dentin b/w base of cavity and pulp decrease of 0.1mm produces more severe inflammation in low speed prep without coolant • With coolant the floor can be brought much closer to pulp (0.3mm) • Pashley Reduction in dentin thickness increases permeability (increase in number and diameter of tubules)
Speeds with 3000 or less and 2,00,000rpm or above are safest with coolant • Speeds between 3000-30,000 rpm are most deleterious even with coolant Riethe • Without use of coolant no high safe speed • At 3000-5000rpm less damage without coolant than at ultra high speed without coolant
HIGH SPEED CUTTING • Burns of dentin • Integrity of pulp threatened • Charred dentinal tubules – susceptible to decay • Ultra high speed should be used for removal of superficial enamel and dentin ,finishing done with very low speed.
With increase in speed of rotation of cutting instrument, not only greater heat is generated but greater vibrations also which affects the pulp • Sears mechanical vibrations may be responsible for protein denaturation of odontoblasts • Causes morphologic changes leading to destruction of cells
Heat and Pressure Factors in production of heat within pulp as a result of cavity preparation are • Depth of preparation • Speed of rotation of bur or stone • Size, shape composition of bur / stone • Amount and direction of pressure on cutting • Amount of moisture • Direction and kind of coolant used • tissue being cut • Length of time instrument in contact.
DRY CAVITY PROCEDURES • Greater trauma than air water spray • Produces both reversible and irreversible changes Prolonged dehydration with air causes • odontoblastic damage, displacement, pulpal edema which cannot be reversed. • Vasodilation • Increase capillary permeability • Above 46°c – irreversible changes – stasis, thrombosis
Initially there is drop of intra pulpal pressure followed by rise due to result of chemical mediators (persistent vasodilation) • Escape of plasma proteins into interstitial fluid ↓ • Lowering of osmotic pressure and accumulation of fluid in pulp chamber.
Kramer (1963),Brown (1978) Enamel temperature increases with dry preparation • May fracture • May effect dentin and then pulp • Breakdown tooth structure at margins • Marginal leakage • Recurrent caries
Nature of cutting instrument :Weiss et al • Greater thermal damage with steel burs, than carbide • With proper cooling carbide burs produces negligible pulp damage • Even with coolant diamond inst are capable of producing damage to pulp this may be related to additional pressure. • Simultaneous inc of rotational speeds and pressure by rotary inst cause temp inc and inc inflammation of pulp • When force above 8 oZ applied – even use of coolant does not resist minimize inflammation ↓ • Displacement of odontoblastic nuclie into tubules
Size of Wheels and burs : • Larger size produce greater damage • Peripheral speed of larger disc is higher than small disc at same rpm • When using large inst greater area is cut. Coolant cannot get to the tooth as readily resulting in more severe reactions • Less severe reactions when smaller size inst used.