Download
1 / 21
210 likes | 517 Views
Materials used to preserve pulp vitality. Calcium hydroxide. The characteristics of calcium hydroxide come from its dissociation into calcium and hydroxyl ions. The action of these ions on tissues and bacteria explains the biological and antimicrobial properties of this substance. .

E N D
Calcium hydroxide • The characteristics of calcium hydroxide come from its dissociation into calcium and hydroxyl ions. • The action of these ions on tissues and bacteria explains the biological and antimicrobial properties of this substance.
it is possible to state that: • 1. Dentin is considered the best pulpal protective, and calcium hydroxide has proved, through numerous studies, its capability of inducing the formation of a mineralized bridge over pulpal tissue. • 2. It is necessary, whenever possible, to provide time for calcium hydroxide paste to manifest its potential of action on the microorganisms present in endodontic infections. The maintenance of a high concentration of hydroxyl ions can change bacteria enzymatic activity and promote its inactivation.
3. The site ofactionofhydroxylionsofcalcium hydroxideincludestheenzymes in thecytoplasmicmembrane. Thismedication has a largeradiusofaction, and thereforeiseffective on a widerangeofmicroorganisms, regardlesstheirmetaboliccapability. • In microbialworld, cytoplasmicmembranes are similar,independently on sort ofmicroorganismmorphological and metabolicalcharacteristics, whichmeansthatthismedication has a similareffect on aerobic, anaerobic, Gram-positive and Gram-negativebacteria.
4. Calcium hydroxideastemporary dressing usedbetweenappointmentspromotesbetterresults on theperiapicalhealingprocessthanthetreatment in oneappointment. • Calcium hydroxideencouragesthedepositionof a hardtissuebridgethatusuallyprotectsthedentalpulp.
calcium hydroxideisanexcellenttherapeuticoptionwhentheclinicalsituationrequirestheuseofpulpcapping agent and intracanalmedication. • Twoeffectsofthismedicationneed to beconsidered, biological and antimicrobialeffects. Thus, otherfactorscanalterthiseffects, liketheinfluenceofvehicles in thisproperties and thetimeofactionfor to expressmicrobialcontrol . • Othersubstanceswithobjectivessimilar to calcium hydroxide, likeMineralTrioxideAgregate and Portland cement, havealsobeenstudied
In the dental pulp, calcium hydroxide has been used as a pulp capping agent because of its ability to stimulate mineralization; • as intracanal dressing it has excellent antimicrobial action, that favor to eliminate microorganisms after cleaning and shaping, to neutralize the remaining toxins, besides maintaining the temporary sealing.
The chemical dynamics of calciumhydroxide as demonstrated by ionic dissociation, characterizes its properties. • The activation of tissue enzymes such as alkaline phosphatase shows mineralizing effects and inhibiting effect on bacterial enzymes, which leads to its antimicrobial property, illustrating the biological qualities of hydroxyl and calcium ions on both tissue and microorganisms
BIOLOGICAL EFFECT • Calcium hydroxideis a strong base obtained through calcination (heating) of calcium carbonate until its transformation into calcium oxide. • Calcium hydroxide is obtained through the hydration of calcium oxide and the chemical reaction between calcium hydroxide and carbon dioxide forms calcium carbonate. It is a white powder with a high pH (12.6) and is slightly soluble in water (solubility of 1.2 g/L, at a temperature of 25oC)36.
The properties of calcium hydroxide come from its dissociation into calcium and hydroxyl ions and the action of these ions on tissues and bacteria explains biological and antimicrobial properties of this substance. • Changes in the biological properties can also be understood through the chemical reactions, since calcium hydroxide, in the presence of carbon dioxide, becomes calcium carbonate (weak acid oxide) and this product does not have calcium hydroxide's biological properties such as the mineralizing capability.
MICROBIAL EFFECT • The mechanism of action of calcium hydroxide on microorganisms can be explained by the influence of pH on growth, metabolism and bacterial cell division. • the hydroxyl ions from calcium hydroxide develop their mechanism of action in the cytoplasmic membrane, because enzymatic sites are located in the cytoplasmic membrane
This membrane is responsible for essential functions such as metabolism, cellular division and growth and it takes part in the final stages of cellular wall formation, biosynthesis of lipids, transport of electrons and oxidative phosphorylation. • Extracellular enzymes act on nutrients, carbohydrates, proteins, and lipids that, through hydrolysis, favor digestion. Intracellular enzymes located in the cell favor respiratory activity of the cellular wall structure. The pH gradient of the cytoplasmic membrane is altered by the high concentration of hydroxyl ions of calcium hydroxide acting on the proteins of the membrane (proteic denaturation).
The effect of the high pH of calcium hydroxide alters the integrity of the cytoplasmic membrane by means of chemical injury to organic components and transport of nutrients, or by means of the destruction of phospholipids or unsaturated fatty acids of the cytoplasmic membrane, observed in the peroxidation process, which is a saponificationreaction
Using mineral trioxide aggregate and calcium hydroxide as a pulp-capping materials • Pulp capping is defined as the placement of a dental material over an exposed pulp to initiate the formation of irritation dentin at the site of injury. Classically, different formulations of calcium hydroxide (CH) have been used. • Today, a newer material is advocated for vital pulp therapy, mineral trioxide aggregate (MTA).
The exposed dental pulp has the capacity to heal when microleakage and bacterial contamination are prevented. Therefore, it appears that an effective pulp-capping material should be biocompatible, that it should provide a biological seal and prevent bacterial leakage.
The pulps capped with MTA or calcium hydroxide showed dentin bridge formation or dentin chips present. Dentin chips may promote or retard healing. A dentin bridge has formed a complete barrier at the exposure site and the pulp is free of inflammations. • The reparative dentin did not originate from severely damaged odontoblasts; instead, undifferentiated cells that migrated from deep regions of the pulp replaced the degenerated odontoblasts. This explains why the reparative dentin is regular when is formed from areas where the odontoblasts remain intact.
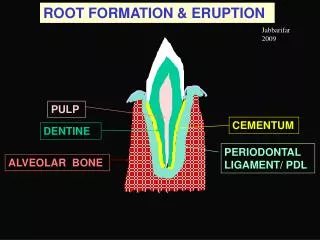
Vital Pulp Therapy • The mechanisms involved in wound healing of pulpal tissue (1) Inflammation (2) CaOH effects (3) Reparative Dentinogenesis (4) Stem Cells (5) Growth Factors • Indirect Pulp Capping • Indications for treatment: Indirect pulp capping is indicted on permanent teeth with immature apices if ALL the following conditions exist:
Tooth has a deep carious lesion that is considered likely to result in pulp exposure during excavation • No history of subjective pretreatment symptoms • Pretreatment radiographs should exclude periradicular pathosis • Patient has been fully informed that endodontic treatment may be indicated in the future
Procedure:Two treatment visits, 6 to 8 months apart. 1st visit; caries biomass is excavated leaving affected dentin adjacent to the pulp. CaOH or MTA is placed over the dentin followed by a base, and the tooth is soundly restored. 2nd visit: the restorative material and the residual caries mass is removed and the tooth restored.
Direct Pulp Capping • Indications for treatment: Direct pulp capping is indicated when all the following clinical conditions exist: • Mechanical exposure of a clinically vital and asymptomatic pulp occurs. • Bleeding is controlled at the exposure site • Exposure permits the capping material to make direct contact with the vital pulp tissue • Exposure occurs when tooth is under rubber dam isolation
5. Adequate seal of the coronal restoration can be maintained. Patient has been fully informed that endodontic treatment may be indicated in the future • Procedure: A radiopaque capping material is place directly over the surface of vital pulp tissue at the site of the pulp exposure followed by a base. The final restoration is placed over the base. The status of the pulp and periradicular tissues should be assessed through periodic recall exams.