Download
1 / 19
310 likes | 754 Views
Development of the cardiovascular system. Begins to function by end of the 3 rd week Necessary in order to meet nutrient needs of rapidly growing embryo Angioblasts arise from: mesoderm Splanchnic & chorionic mesenchyme yolk sac & umbilical cord Give rise to blood & blood vessels.

E N D
Development of the cardiovascular system • Begins to function by end of the 3rd week • Necessary in order to meet nutrient needs of rapidly growing embryo • Angioblasts arise from: • mesoderm • Splanchnic & chorionic • mesenchyme • yolk sac & umbilical cord • Give rise to blood & blood vessels
Angioblasts • AKA hemopoietic mesenchyme differentiates into the blood islands • Central cells of blood islands differentiate into blood and blood cells • Lined with endothelium
Formation of blood cells • Yolk sac-4th week • Body mesenchyme & blood vessels-5th week • Liver-6th week • Spleen, thymus, lymph glands-2-3 months • Bone marrow- 4th month • There is overlap in production sites
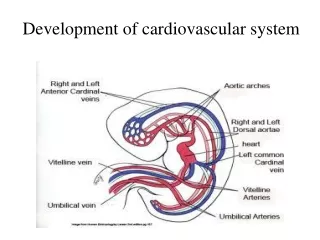
Development of Main Blood Vessels • First indication of paired blood vessels • 3 week old embryo • Embryonic period (4-8 weeks) • By end of embryonic period the main organ systems have been established • Appear as solid cell clusters which acquire a lumen & form a pair of longitudinal vessels • Dorsal aorta • Aortic arches • Continue anteriorly and run ventrally • Heart primordia • Continue posteriorly
Venous system at 4 weeks • 3 systems of paired veins drain into heart • Vitelline veins • Returning blood from yolk sac • Umbilical veins • Bring blood from the chorion and placenta • Cardinal veins • Returning blood from various parts of the body • vascular system
Arterial system at end of 4 weeks • Four pairs of aortic arches have appeared • Dorsal aorta have fused throughout much of their length descending aorta
Development of the heart • Starts as two thin walled endocardial tubes • Caudal continuation of the first aortic arches • Endocardial heart tubes • Begin to fuse to form a single tube • As heart tube fuses • Surrounding mesenchyme thickens to form • Myocardium • Epicardium • Tubular heart elongates and develops dilations or sacculations • Primordia of Truncus, Bulbus, Ventricle, Atrium, Sinus (SI) • heart development (adam) • development of the heart • actual mouse embryo
Primitive heart • Primordia (SI) (Cranially Caudally) (A V) • Truncus • Continuous cranially with first pair of aortic arches • Bulbus • Ventricle • Both bulbus and ventricle grow faster than other parts which causes S shape bend animation • Atrium • Sinus • Receives venous return from • Umbilical, Vitelline & Common cardinal veins
Primitive heart • As primitive heart bends the atrium and sinus come to lie dorsal to the bulbus & ventricle • Reversal of original cranio-caudal relationship • Atrial portion being paired becomes one • Atrioventricular junction remains narrow • Form an atrioventricular canal • Connecting atrium with the ventricle
Primitive heart (cont) • At the end of loop formation, the smooth inner heart surface begins to form the primitive trabecullae in the ventricle • Atrium & bulbus remain temporarily smooth • Sinus maintains it’s paired condition longer than any other portion of heart tube • Contraction begins by day 22 • Initially ebb & flow unidirectional flow • By end of 4th week, rhythmic contraction
Formation of cardiac septa • Begins around middle of 4th week & completed by end of 6th week • Two methods • Tissue growth • Two of more actively growing masses of tissue which approach each other in the same plane, fuse to divide a single chamber into two • Overgrowth • Involves growth of a chamber at all points except for a narrow strip which fails to grow • Leaves a small canal connecting the two chambers
Cardiac Septum • Atrioventricular septum (during 4th week) • Bulges form on dorsal & ventral walls of AV canal AKA endocardial cushion septum • Atrial septa (end of 4th week) • Sickle-shaped crest grows from roof of common atrium in the direction of the endocardial cushion • Septum primum • As right atrium grows & incorporates part of the sinus • Septum secundum associated with foramin ovale (oval foramin) • Ostium primum • Opening between septum and endocardial cushion which closes by growth of endocardial cushion • Ostium secundum superior in septum primum
Foramin ovale (FO) • Shunts blood from Right to left atria via ostium secudum • Mostly blood returning via inferior vena cava • Bypasses lungs in fetus • Associtated with septum secundum • At birth FO pressed against septum primum which seals the opening
Septal formation • Ventricular septum (starts by end of 4th week) • Expansive growth of ventricle laterally & ultimate fusion of the medial walls starts the formation of the Muscular Interventricular Septum near apex • Communication btw ventricles below cushion • Closed by membranous IV septum at end of 7th week • Septum of the truncus & bulbus • Continous paired ridges fuse • Form a spiral septum (aorticopulmonary septum) • Cavum aorticum LV • Cavum pulmonare RV • Two cava eventually separate forming acending aorta & pulmonary trunk • image
Congential malformations • Acardia • Absence of heart • Only occurs in conjoined monozygotic twins • 1:35,000 • Ectopic Cordis • Heart is located through a sternal fissure into: • Into the neck • Down through a diaphragmatic hernia into a exomphalocoele • Protruding outside chest • Dextra thoracic ectopia • Limited life expectancy
Congenital Malformations • Dextracardia • Heart is located in right hemithorax • Most cases associated with situs inversus • Heart, great vessels, other thoracic & abdominal organs may present a mirror image of the norm. • 1:10,000 • Known to occur with other anomolies • Duodenal atresia • Agenesis of spleen • Spina bifida • Isolated cases rare (1:900,000)
Septal Defects • Atrial Septal Defect • Well tolerated into adult life • Problem in old age • May be combined with rarity of other cardiac anomalies • Prenatal Closure of the interatrial shunt • Enlargement of right atrium & ventricle • Causes hypoplastic left side • Death soon after birth • Ventricular Septal Defect • About ½ of all cases of congestive heart failure show a VSD • Uncomplicated form considered harmless • Harsh systolic murmur with no cyanosis • 6:10,000
Tetralogy of Fallot • Pulmonary stenosis • VSD • Overriding Aorta • Right Ventricular hypertrophy • Life expectancy 12 years • Major symptom is cyanosis • Paroxysmal dyspnea on exertion is common • Above symptoms may lead to unconsciousness & paralysis
Trilogy of Fallot • Pulmonary Stenosis • ASD • Right ventricular hypertrophy