Download
1 / 99
1.1k likes | 1.58k Views
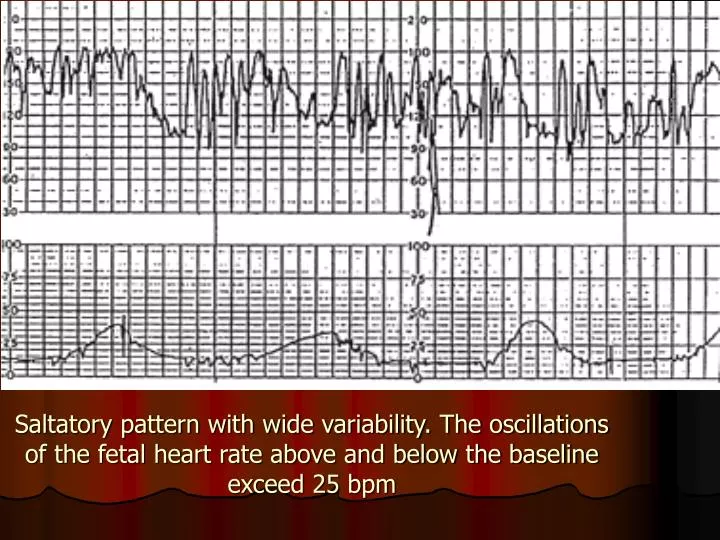
Saltatory pattern with wide variability. The oscillations of the fetal heart rate above and below the baseline exceed 25 bpm.

E N D
Saltatory pattern with wide variability. The oscillations of the fetal heart rate above and below the baseline exceed 25 bpm
Fetal tachycardia with possible onset of decreased variability (right) during the second stage of labor. Fetal heart rate is 170 to 180 bpm. Mild variable decelerations are present.
Fetal tachycardia that is due to fetal tachyarrhythmia associated with congenital anomalies, in this case, ventricular septal defect. Fetal heart rate is 180 bpm. Notice the "spike" pattern of the fetal heart rate.
Early deceleration in a patient with an unremarkable course of labor. Notice that the onset and the return of the deceleration coincide with the start and the end of the contraction, giving the characteristic mirror image.
Nonreassuring pattern of late decelerations with preserved beat-to-beat variability. Note the onset at the peak of the uterine contractions and the return to baseline after the contraction has ended. The second uterine contraction is associated with a shallow and subtle late deceleration.
Late deceleration with loss of variability. This is an ominous pattern, and immediate delivery is indicated.
Variable deceleration with pre- and post-accelerations ("shoulders"). Fetal heart rate is 150 to 160 beats per minute, and beat-to-beat variability is preserved
Severe variable deceleration with overshoot. However, variability is preserved.
Late deceleration related to bigeminal contractions. Beat-to-beat variability is preserved. Note the prolonged contraction pattern with elevated uterine tone between the peaks of the contractions, causing hyperstimulation and uteroplacental insufficiency. Management should include treatment of the uterine hyperstimulation. This deceleration pattern also may be interpreted as a variable deceleration with late return to the baseline based on the early onset of the deceleration in relation to the uterine contraction, the presence of an acceleration before the deceleration (the "shoulder") and the relatively sharp descent of the deceleration. However, late decelerations and variable decelerations with late return have the same clinical significance and represent nonreassuring patterns. This tracing probably represents cord compression and uteroplacental insufficiency.
Pseudosinusoidal pattern. Note the decreasedregularity and the preserved beat-to-beat variability
List 6 Causes of Severe Fetal Bradycardia ? • Prolonged cord compression • Cord prolapse • Tetanic uterine contractions • Paracervical block • Epidural and spinal anesthesia • Maternal seizures • Rapid descent • Vigorous vaginal examination
list 6 Causes of Severe Fetal Bradycardia ? • Prolonged cord compression • Cord prolapse • Tetanic uterine contractions • Paracervical block • Epidural and spinal anesthesia • Maternal seizures • Rapid descent • Vigorous vaginal examination
What is the Signs of Nonreassuring Variable Decelerations that Indicate Hypoxemia ? • Increased severity of the deceleration • Late onset and gradual return phase • Loss of "shoulders" on FHR recording • A blunt acceleration or "overshoot" after severe deceleration • Unexplained tachycardia • Saltatory variability • Late decelerations or late return to baseline • Decreased variability
what is the Nonreassuring patterns in the CTG? • Fetal tachycardia • Fetal bradycardia • Saltatory variability • Variable decelerations associated with a nonreassuring pattern • Late decelerations with preserved beat-to-beat variability
what is the Ominous patterns of the CTG? • Persistent late decelerations with loss of beat-to-beat variability • Nonreassuring variable decelerations associated with loss of beat-to-beat variability • Prolonged severe bradycardia • Sinusoidal pattern Confirmed loss of beat-to-beat variability not associated with fetal quiescence • medications or severe prematurity
Emergency Interventions for Nonreassuring Patterns • Call for assistance • Administer oxygen through a tight-fitting face mask • Change maternal position (lateral or knee-chest) • Administer fluid bolus (lactated Ringer's solution) • Perform a vaginal examination and fetal scalp stimulation When possible, • determine and correct the cause of the pattern Consider tocolysis (for uterine tetany or hyperstimulation) • Discontinue oxytocin if used Consider amnioinfusion (for variable decelerations) • Determine whether operative intervention is warranted and, if so, how urgently it is needed
Causes of Fetal Tachycardia • Fetal hypoxia • Maternal fever • Hyperthyroidism Maternal or fetal • anemia Parasympatholytic drugs • Atropine • Hydroxyzine (Atarax) • Sympathomimetic drugs • Ritodrine (Yutopar) • Terbutaline (Bricanyl) • Chorioamnionitis • Fetal tachyarrhythmia • Prematurity
This patient was induced with prostin E2 gel. One hour after administration the cardiotocograph (CTG) was recorded. • 1.What CTG abnormalities do you see? • Reduced baseline variabilityLate deccelerationsExcessive uterine activity (approximately 7 in 10 minutes) • 2.What is the diagnosis? • Uterine hyperstimulation leading to fetal comprimise
3.What is your management? Move the patient onto her left side to reduce the risk of aortocaval compression. Facial oxygen may improve fetal oxygenation.Use of an intravenous tocolytic agent will reduce the uterine activity. Suitable drugs include salbutamol or ritodrine, both of which are beta-2 agonists.The resulting CTG is shown below.
Q732 Y OLD PG who present at 38 week gestation with reduce fetal movement CTG done,show
1.What abnormality are shown in the CTG? • 2.What will be the most likely plan of management? • 3.further CTG show persistent of this pattern what will you advice? • 4.if she went into labour ,what must you do?
1.What abnormality are shown in the CTG? • 1.Fetal tachycardia with possible onset of decreased variability • 2.What will be the most likely plan of management? • Admit into the labour word with continuous monitoring • 3.further CTG show persistent of this pattern what will you advice? • Delivery by CS if cervix un favorable orARM if cervix favorable,and thin start syntocinon • 4.if she went into labour ,what must you do? • Ensure that fetus monitored continuously and perform a fetal blood sample if this pattern persist
Q#139y old G3P2 admitted in active labour after 3hr CTG show
1.Describe the CTG finding? • 2.what is the next action you will do? • 3.on examination cervix was fully dilated head at +2 station with caput ++ CTG persist the same. how you are going to manage this patient? 4.What other indication for its use? 5. What 6 condition must be fulfilled before the application of this instrument? 6.what 4 complication may arise from use of this instrument?
1.Describe the CTG finding? • Late deceleration with loss of variability. This is an ominous pattern, and immediate delivery is indicated • 2.what is the next action you will do? • Put the patient in lateral side ,give oxygen ,fast iv drip ,and examine the patient to decide about the mode of the delivery • 3.on examination cervix was fully dilated head at +2 station with caput ++ CTG persist the same. how you are going to manage this patient? Immediate delivery is indicated ,forceps delivery is appropriate for this pt
2.Uterine artery Doppler is a promising technique for assessment of the level of risk of pre-eclampsia and IUGR. Doppler ultrasound provides a non-invasive method of assessing the utero-placental circulationIn normal pregnancy , impedance to flow in the uterine artery decreases with gestation and this presumably reflects the trophablastic invasion of the spiral ateries and their change into low resistance vesselsThe uterine artery is a branch of the internal iliac artery close to the bifurcation of the common iliac. Colour flow Doppler is the method of choice for accurate screening of uterine artery waveforms.
The resistance index (RI) is the most commonly used index to measure the uterine artery flow as it is unlikely to have absent or reverse end Diastolic (EDF) flow. Although the pulsatility index (PI) can also be used 3.High resistance waveforms in the uterine artery with early diastolic notching in the second trimester are asssociated with the later development of pre-eclampsia, IUGR, placental abruption and intra-uterine death. 4. notches of the uterine artery waveform with a high RI, hold the most risk of complicated pregnancies, although it is still to be established wether the notch or the high RI is the best indicator of poor outcome 5. Systole (Sys) and diastole (D) are identified in green Note that diastole is less at 20 weeks (yellow ellipse) than at 36 weeks (red ellipse). 6. This illustrates absent diastolic flow during diastole. When this occurs there is abnormal resistance in the placenta which results in a marked decrease in blood flow from the fetus to the placenta.
7. Color Doppler of umbilical cord insertion • 8. Color Doppler and spectral Doppler of ovarian artery • 9.Color Doppler and spectral Doppler of umbilical artery • 10. Color Doppler of left ventricular outflow tract • 11. Color Doppler of umbilical cord • 12. Chromosome pattern of a person with Down's syndrome. Arrow points to an extra chromosome No.21
What is the Signs of Nonreassuring Variable Decelerations that Indicate Hypoxemia ? • Increased severity of the deceleration • Late onset and gradual return phase • Loss of "shoulders" on FHR recording • A blunt acceleration or "overshoot" after severe deceleration • Unexplained tachycardia • Saltatory variability • Late decelerations or late return to baseline • Decreased variability
what is the Nonreassuring patterns in the CTG? • Fetal tachycardia • Fetal bradycardia • Saltatory variability • Variable decelerations associated with a nonreassuring pattern • Late decelerations with preserved beat-to-beat variability
what is the Ominous patterns of the CTG? • Persistent late decelerations with loss of beat-to-beat variability • Nonreassuring variable decelerations associated with loss of beat-to-beat variability • Prolonged severe bradycardia • Sinusoidal pattern Confirmed loss of beat-to-beat variability not associated with fetal quiescence • medications or severe prematurity
Emergency Interventions for Nonreassuring Patterns • Call for assistance • Administer oxygen through a tight-fitting face mask • Change maternal position (lateral or knee-chest) • Administer fluid bolus (lactated Ringer's solution) • Perform a vaginal examination and fetal scalp stimulation When possible, • determine and correct the cause of the pattern Consider tocolysis (for uterine tetany or hyperstimulation) • Discontinue oxytocin if used Consider amnioinfusion (for variable decelerations) • Determine whether operative intervention is warranted and, if so, how urgently it is needed
Causes of Fetal Tachycardia • Fetal hypoxia • Maternal fever • Hyperthyroidism Maternal or fetal • anemia Parasympatholytic drugs • Atropine • Hydroxyzine (Atarax) • Sympathomimetic drugs • Ritodrine (Yutopar) • Terbutaline (Bricanyl) • Chorioamnionitis • Fetal tachyarrhythmia • Prematurity