Download
1 / 31
310 likes | 329 Views
Obesity and Insulin Resistance Are the Central Issues in Prevention of and Care for Comorbidities. Elisabeth Govers, RD Dutch Knowledge Centre for Dietitians on Overweight and Obesity. Disclaimer. E. Govers declares to have no competing interests.

E N D
Obesity and Insulin Resistance Are the Central Issues in Prevention of and Care for Comorbidities Elisabeth Govers, RD Dutch Knowledge Centre for Dietitians on Overweight and Obesity
Disclaimer • E. Govers declares to have no competing interests. • Data have been collected in primary care practices in the Netherlands by dietitians
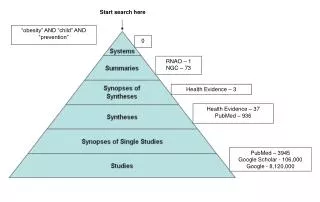
Content • The obesity dilemma • The cause of insulin resistance • The relationship of IR with comorbidities • The guideline for the management of insulineresistance • Conclusions and recommendations
The obesity curve Comorbidities BMI 25 27 30 35 40 45 50 BMI low, few comorbidities, fairly easy to lose weight BMI high, manycomobidities and hard to lose weight
The obesity curve Comorbidities Low carb diet BMI 25 27 30 35 40 45 50 There is a point of no return, afterwhich only bariatricsurgery helps
The obesity dilemma • Obesity levels are risingthroughout the world • Treatment is consideredfairly easy: justeatless and exersize more……….. • Treatment canbeadministeredbyanyone with a lowereducation in health care • Treatment canbedoneby commercial parties • There is no way to escape marketing of unhealthy foods
Cohort patients in primary care 2005: Baseline measurement of dietary practices 2007: Letter of invitation Journal Dutch Ass. Of Dieticians 36 practices responded 12 practices responded 16 practices declined participation 4 practices declined participation 20 practices entered study: 140 dietitians 8 practices entered study : 50 dietitians 2007: 28 practices entered study; 190 dietitians; 3000 questionnaires distributed 32 dieticians declined Baseline: 1549 questionnaires returned by 158 dietitians. Missing data of 81 patients: 12 male (14.8 %); 69 female (85.2 %) After six months: 1468 adults; 445 male (30.3%); 1023 female (69.7%) questionnaires of adults returned by 140 dietitians from 24 practices with valid baseline BMI. Still in treatment after 6 months: n = 521; 151 male (29.1%); 370 female (70.9%) Patient dropped out: n = 469; 128 male (27.8%); 341 female (71.9%) Treatment has ended between 1 and 6 months: n = 478; 166 male (34.4%); 312 female (65.6%).
Percentage weight loss after 6 months Missing 454
Diet related to weight loss after 6 months* >5% weight loss • Low energy diet 29,1% • RGV 34,2% • Low fat diet 28,6% • Low carb diet 46,1% >5% loss of waist circumference • Low energy diet 40% • RGV 38% • Low fat diet 25% • Low carb diet 57% * 57% comorbidities Govers et al, 2008 <3% or no weight loss • Low energy diet 41,7% • RGV 35,9% • Low fat diet 28,8 • Low carb diet 28,8% <3% loss of waist circumference • Low energy diet 37,9% • RGV 35,8% • Low fat diet 62% • Low carb diet 42,8
Weight loss on low carb diet • Feinman RD, Pogozelski W, Astrup, Bernstein RK, Fine EJ, Dashti HM et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition; 31-1, 2015: 1–13. • Shai I et al., Weight loss with a low carbohydrate, Mediterranean, or low fat diet. New England Journal of Medicine. 2008; 359): 229-41. • Ajala O. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. American Journal of Clinical Nutrition 2013; 97: 505-16. • Westerterp-Plantenga MS, Nieuwenhuizen A, Tomé D, Soenen S, Westerterp KR. Dietary protein, weight loss, and weight maintenance. Annu Rev Nutr. 2009;29:21-41. doi: 10.1146/annurev-nutr-080508-141056. Review. • Layman DK, Walker DA. Potential Importance of Leucine in Treatment of Obesity and the Metabolic Syndrome 1-3, American Society for Nutrition 2008. • Coumans T, Malcontent V. What is the effect of a low carb diet on health of patients with type 2 diabetes with overweight, insulin resistance and insulin therapy? HEI Arnhem& Nijmegen 2013. • Verkoelen H. Echt afvallen doe je zo. Andere gezonde voeding, minder koolhydraten. Uitgeverij Prima Vita,2012. ISDN 9090272437.
Proef diabetes: spectaculair resultaat Published: 3-13-2016 3 Laatst gewijzigd op: 13 - 3 - 2016 19:45 Introductie Meer dan tweederde van de 55 patiënten met diabetes type 2 die deelnamen aan een proef van VGZ, Voeding Leeft en zorggroep Synchroon hoeven geen of veel minder diabetesmedicatie te gebruiken. Dit blijkt uit de eerste tussentijdse resultaten van de proef ‘ Keer Diabetes Om’ in Uden, waarbij voeding als medicijn wordt gebruikt. Een Vandaag besteedde vrijdagavond uitgebreid aandacht aan dit onderwerp met Ab Klink als studiogast. Pagina - inhoud In veel gevallen blijkt diabetes om te keren als mensen zelf, geholpen door hun artsen, voor andere voeding en voor meer beweging kiezen. Hiermee krijgt de patiënt weer de regie over zijn eigen gezondheid. Zinnige zorg De proef past in de beweging die w e met VGZ maken naar zinnige zorg. Artsen geven daarbij aan wat de beste zorg is en wij ondersteunen dat ten behoeve van de patiënt. Ab Klink: "Vaak gebruiken mensen onbewust te veel medicijnen. Ik vind de eerste uitkomsten van dit groepsprogramma echt sp ectaculair. Dat is in de eerste plaats natuurlijk goed nieuws voor de patiënt zelf, maar natuurlijk ook voor de premiebetaler: het verbetert de kwaliteit van leven, het verbetert de kwaliteit van de zorg en het verlaagt de zorgkosten. Bij een positief eind resultaat zullen we het Groepsprogramma per 1 januari 2017 op landelijke schaal inkopen en opnemen in het basispakket.” De proef loopt nog enkele maanden door. Deze week is er weer een nieuwe lichting begonnen aan het Groepsprogramma onder begeleiding van een lifestylecoach, diëtist, kok en praktijkondersteuner van de huisarts. Trend: jaarlijkse kosten € 20 miljard in 2025 Bijna 1 miljoen mensen in Nederland hebben diabetes type 2. Ieder uur sterft er in Nederland iemand aan de gevolgen van diabetes. Med icatie bestrijdt slechts enkele symptomen van diabetes, maar geneest de patiënt niet. De hoge kosten die de huidige aanpak van diabetes type 2 met zich meebrengt, maakt het een economisch probleem van nationale omvang. De kosten zijn nu al ruim 10 miljard euro per jaar (type 1 en 2 samen) en lopen bij de huidige trend op naar 20 miljard euro jaarlijks in 2025. Bekijk EENVANDAAG 11 maart 2016 terug New developments in diabetes care
The adipocyt in obesity McArdle, 2013 Hyperfagia (carbs, sat fats) leads to positive energy balance, enlarges adipocytes and accumulation of fat in the abdomen, and finally to hypoxia and metaflammation: insulin resistance
The adipocyt and adipocytokines Fruhbeck, 2001
Clinical parameters • Hypertension • Dyslipidemia • Low HDL • Elevated LDL and triglycerides • PCOS (policysticovariansyndrome) • NAFLD (non alcoholicfattyliver disease) • Impaired glucose tolerance and type 2 diabetes • Osteo artritis • Elevated oestrogeen • Fertilityproblems • Low testosterone • Reducedthyroicglandfunction • Sleep apnoea • Gout • Increased activity of mast cellsin the duodenum • Fatigue • Vit D deficiency • Emotionalinstability • Increased risk of infections
Basic problem • The high insulinproductioncauses more fat storage and prevents weight loss • Allcomorbidities are interconnected • Substantial weight loss on diets with normalcarbohydrate content is fairlyimpossible • Prevention of chronic disease shouldbe the central issue: • weight + waist
Additonalproblems • Patients have a long history of weight loss attempts • Diet contains up to 80% carbohydrates, protein malnourished • Patients have a constant appetite, loss of control • Physical conditition is bad
Obesity needs management byexperienced & highly qualified health professionals Role of the dietician EFAD strongly believes that dieticians are in a key position to influence the promotion of a healthy lifestyle. They are educated in nutrition, health, counselling and behavioural strategies and are actively involved in public health, health promotion, clinical treatment, disease management and research. Dieticians have the skills to interpret and communicate the theoretical knowledge to enable individuals to make appropriate choices about food and healthy lifestyle and to teach people how to sustain healthy behaviour. EFAD Position paper on obesity (2011):
How to treat insulin resistance • 10-15% weight loss + loss waist circumference through low carb, high protein diet • Exercise: up to one hour per day: • Brisk or nordic walking, cycling, swimming, fitness (only 2-3 x per week) • Endurance training has direct influence on reduction of ADP! • In T2 diabetes endurance exercise can be helpful • Postpone medication as much as possible. Metformin sometimes has beneficial effect
Treatment Goals • Improving insuline sensitivity through carbohydraterestriction • Optimalisation of othermacronutrients: protein, mono unsatured fats, omega-3 fat • Improvingallphysiological and bloodvalues • 10-15% weight loss (20/25% in morbide obesity); weight maintenance 2-5 years • Loss of :10% waistcircumference • Maximum satiation and satiety through optimalquantities of protein, fat and fibre
Treatment Goals 7) Sustaining or increase of free fat mass 8) Optimalintake of vitamins and minerals, suppletion of 1 x ADA, vit D suppletion 400/800 IE 9) Exersize with sufficient intensity and muscle building: build up to 1 hour per day* 10) Improvementof sleep 11) Improvement of quality of life (mentally and conditionionally) * Ifpatient has notexersizedfor a long time: advicewalking, build up from 15 minutes to 1 hour per day
Criteria carbohydraterestriction Table based on Feinman et al (2015) & Ten Hoor-Aukema en Schweitzer (2000)
Benefits • High protein meals give more satiation and postpone appetite for hours: easier not to eat in between meals and uphold the diet. • Patients start to feel better (more energy) • Glucose values and other parameters drop • Patients are able to control their appetite which improves self-confidence and prevents craving • A diet rich in protein and low in carbohydrates is good for long-term weight maintenance.
Long-term sustainability • Patients need teaching howtheir body worksdifferently to help themsustain new food habits • ´home-sickness´ for carbohydrates is a big pitfall • Large carb intake is usuallysociallyembedded • Obesogenic environment is a constant challenge • Easy accessability to low carb food is needed
Conclusions • A shift of paradigm is needed: fromwaitingtillcomorbiditiesoccur to actively telling individuals (and families) to lose weight • Weight loss: carb protein • Selfmanagement with specialisedHPs as coach, family treatment • Obesogenic environment must improve: different foods, more exercise, less stress
Thank you! Questions www.kdoo.nlinfo@kdoo.nl