Download
1 / 37
400 likes | 429 Views
Explore the intricate processes of thyroid physiology, from iodide turnover to hormone biosynthesis and release. Learn about TH actions on body tissues and how disorders like hypothyroidism and hyperthyroidism affect health.

E N D
Dr. Mohammed Kalimi Thyroid Physiology
Iodide Turnover • Input = Output • 500 μg Iodide = Renal excretion =480 μgI- (Daily dietary) Stool excretion= 20 μg I -
Biosynthesis of TH • 1. Iodide pump or trap: • Transport of iodide into the gland against electro chemical gradients by Na+ -I- cotransport (symport) • ↑ Na-K ATPase and TSH • Inhibition by Sodium thiocyanate and Perchlorate
T/S Ratio • Normal T/S 20:1 • TSH stimulation 100:1 • Hypophysectomized (no TSH) 1:1
Biosynthesis of TH • 2. Conversion of Iodide to Iodine 2I - I2 • H2O2 sustrate and thyroid peroxidase enzyme • ↑ TSH and inhibited by PTU and methimazole
Biosynthesis of TH • 3. Organification: Formation of MIT and DIT by iodination of tyrosyl residue of TG • 4. Coupling: MIT + DIT = T3 DIT + DIT = T4 Organification and coupling are caralyzed by thyroid peroxidase and require hydrogen peroxide and TSH
Administration of large quantities of Iodide (2 mg or more) • TH synthesis due to • expression of Na-I symporter • enzyme peroxidase genes
T3 and T4 Plasma bound T4 = 99.97% Plasma free T4 = 0.03% Plasma bound T3 = 99.7% Plasma free T3 = 0.3%
T3 and T4 • Ten times (of the total) T3 in the blood is free Compared to T4 • Plasma half life of T3 = 1 day • Plasma half life of T4 = 7 days • T3 is two to three times more biologically potent than T4
TH blood binding proteins • Thyroxine binding globulins (TBG): binds to about 70% total T4 and 50% total T3 • Thyroxine binding prealbumin (TBPA): binds 20% of total T4 ( no binding to T3) • Albumin : binds 10% of total T4 and 50% of total T3
Degradation of T4 • 1. Conversion of T4 to T3 (T4 5’ Deiodinase T3) about 35% • 2. Conversion of T4 to rT3 (T4 5 Deiodinase rT3) about 45% • 3. T4 metabolised by cojugation or oxidative deamination : about 20%
Reverse T3 • Physiological role unknown • Levels ↑ with chronic illness, calorie deprivation, β blockers and corticosteroids
Thyroid Physiology • Acts on most tissues • Action –slow in onset and long in duration • TH is not necessary for life, improves quality of life
TH Actions • 1. Growth and Development • 2. Metabolic • 3. Neural • 4. Cardiovascular
TH Actions • Normal growth (↑GH)and development (bone, skeletal and brain) • Congenital deficiency ; cretinism • Dwarf stature (bone remains infantile ), mental retardation
TH Actions • Metabolic: ↑ BMR, ↑ O2 consumption, ↑ heat production, ↑ mitochondrial ATP synthesis. • Acute response to cold by ↑ BMR, ↑ heat production, ↑ catecholamines, ↑ lipolysis, ↑ cardiac adjustments, ↑ muscular activity • Chronic cold: ↑ conversion of T4 to T3
TH Actions • ↑ Carbohydrate, protein and lipid metabolism • ↑ Gluconeogenesis, ↑ Glycolysis, ↑ absorption of carbohydrates from the GI tract • Negative nitrogen balance (↑ protein turnover) • ↑ Lipolysis, FFA synthesis and oxidation • Total cholesterol and LDL
TH Actions • Neural: Promotes normal neuronal development • Cardiovascular effects: ↑ heart rate and strength of the heart beat, ↑ ventilation and cardiac output • ↑ Cardiac β receptors
TRH • Tripeptide • Synthesized and released from hypothalamus • ↑ T3,T4, anterior pitutary TRH receptors, TSH
TSH • α subunit identical with LH, FSH, hCG • β subunit is specific to TSH • Plasma T1/2= 1 hour • Plasma TSH levels = 0.5-5.0 μU/ml • ↑ TSH, ↑ cold, ↑ TRH, ↑ leptin • TSH, sleep, fasting and ↑ somatostatin
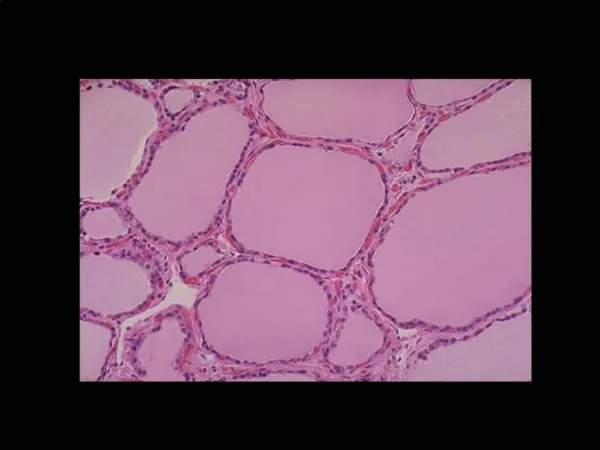
Goiter ( enlargement of TH gland) • Prolonged and excessive TSH stimulation of TH gland • Euthyroid Goiter: Iodide deficiency, ↑ TSH to compensate TH • Hyperthyroid Goiter: over secretion of TSI (thyroid stimulating immunoglobulin) which mimics TSH, ↑ TSI, ↑TH • Hypothyroid Goiter: Administration of drugs such as PTU, perchlorate, thiocyanate, TH,↑ TSH
TH : Clinical tests • Measurement of plasma total T3 and Total T4 • Measurement of TSH • Normal values= 0.5-5.0 micro units/ mL of blood • Elevation in serum TSH is the most sensitive measure for primary hypothyroidism
TH: Clinical tests • TSH above 5.0 (hypothyroidism) treatment with thyroxine • TSH below 0.5 (hyperthyroidism), radiation treatment plus thyroxine (T4)
TH Clinical • In deficiency state: Hypothyroidism • Overactivity: Hyperthyroidism
Hypothyroidism • Primary disease: Thyroid failure (surgical, immune or iodide destruction of thyroid gland) • Secondary disease: Pituitary (TSH deficiency) or hypothalamus (TRH deficiency)failure • Defective TH receptors • Myxedema • Cretinism
Symptoms of hypothyroidism • Decreased BMR , decreased pulse rate and vitality • Increased plasma cholesterol and LDL • Growth failure, weight gain, constipation • Dry scaly thickened skin, cold intolerance • Sluggishness, hoarse voice, lethargic, puffy eyelids, enlragement of tongue • Depression and insomnia
Hyperthyroidism • Graves’ disease (Thyrotoxicosis) • ↑ TSI, ↑ T3,T4, TSH
Symptoms of hyperthyroidism • ↑ BMR • Plasma Cholesterol and LDL • ↑ Cardiac output, ↑ heart rate and ↑cardiac beta receptors, congestive heart failure • ↑ Body heat, sweating and vasodialation • Osteoporosis (negative calcium balance) • Hyperkinetic and psychotic behavior • ↑ GI malfunctions and weight loss • Neuro muscular-fatigue,hyperactive reflexes • Eye discomfort, marked protrusion of eyes (exophthalamos)
Pregnancy and TH • Pregnancy, ↑ Estrogen, ↑TBG, ↑Total plasma T3 and T4