Download

1 / 56
560 likes | 727 Views
HIV/AIDS and older persons. History, prevalence and impact in South Africa. Sebastiana Kalula Institute of Ageing in Africa Groote Schuur Hospital University of Cape Town South Africa. The HIV/AIDS epidemic.

E N D
HIV/AIDS and older persons History, prevalence and impact in South Africa SebastianaKalula Institute of Ageing in Africa Groote Schuur Hospital University of Cape Town South Africa
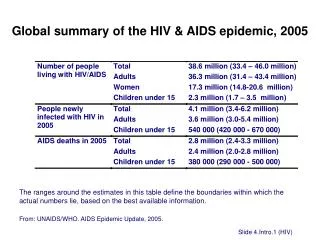
The HIV/AIDS epidemic • Two thirds (67%) of the 33 million people worldwide living with HIV and AIDS are in sub-Saharan Africa • Heterosexual transmission is the predominant mode of the spread of the HIV virus in the sub-continent • Other specific modes of transmission are sex work, intravenous drug use and male sex UNAIDS, 2009
Factors contributing to spread of HIV: • Poverty • Social inequality and political instability • High levels of sexually transmitted infections • Low status of women • Sexual violence • High mobility levels (migrant labour) • Limited and inequitable access to quality medical care • Poor leadership in response to the epidemic
History of HIV and AIDS in South Africa • South Africa has had a turbulent political past • The epidemic affects people from all walks of life • Early history of HIV in the country largely confined to homosexual men • AIDS was viewed as a homosexual disease
Cont. • Wider population thus largely ignored the risks of contracting the virus • Apartheid government excused itself from responding proactively • Haemophiliacs became infected through infected blood and blood products • Moralisation of the epidemic
Cont. • Black South Africans were first diagnosed with the disease in 1987 (among mine workers) • Mine workers are vulnerable to HIV infection due to high levels of mobility (migrant labour) • The industry is largely dependent on local and regional migrant workers • Operates in inhospitable locations family separation and isolation
Cont. • In the 1990s the South African epidemic was linked to the wider continental epidemic with dominant strains of HIV previously found in Central Africa • Areas of high prevalence were located along long-haul truck routes leading into bordering countries • Heterosexual transmission has become by far the dominant transmission route
First national response • Early nineties saw AIDS start to make its way onto the national agenda in South Africa • Creation of the National AIDS Coordinating Committee of South Africa (NACOSA) in 1992 • In the turbulent political climate many groups attached conspiracy theories, and unfounded political and racial motivations to the spread of HIV
Increased prevalence antenatal clinics Increased infant mortality No Mother-to-Child Transmission Prevention Programme (MTCTP)
Cont. • In 2001 the South African government implemented an MTCTP programme after being taken to court • In 2003 it produced an Operational Plan for the rollout of antiretroviral treatment, with treatment starting in 2004
Social and economic impact • In 2009 average life expectancy in SA was 54 years; without AIDS, it is estimated it would have been 64 • Between 1990 and 2003 when HIV prevalence in SA increased dramatically, the country fell by 35 places in the Human Development Index Stats SA, 2009
Population ageing South Africa Stats SA, 2009 UNDP, 2006
Population ageing • Size of black older population will increase dramatically • Size of white older population will diminish proportionately • Black older persons: • Disadvantaged across the life course • Largely poor • Lack medical insurance • Dependent on public health and welfare services
Population ageing South Africa faces accelerated population ageing • HIV/AIDS epidemic high mortality in infants, children, young adults • Diminished work force and reduced tax base • Diminished support for the now young grandmothers, who will grow old
HIV prevalence in South Africa • Three national population-based surveys conducted by the Human Sciences Research Council (HSRC) • HIV prevalence in the age group 2+ years in South Africa was 11.4% in 2002, 10.8% in 2005 and 10.9% in 2008 • Prevalence is heterogeneous in South Africa’s provinces, ranging from 15.8% in KwaZulu-Natal to 3.8% in the Western Cape
Factors predisposing to HIV infection: • Early sexual debut – entry into sexual relationships before age 15 years • Older sexual partners (five or more years) • Unequal power dynamics, with vulnerable young girls and wives unable to negotiate condom use • High turnover of partners, or multiple partners
In 2009, SA had an estimated overall HIV prevalence of 10.6% and 5.21 million people are living with HIV • In age group 15-49 years, 17% are HIV positive • In 2009, estimated new HIV infections were 413 000, 59 000 of which were among children • There are approximately 1.91 million AIDS orphans in the country Stats SA, 2009
Prevalence in older persons • Prevalence rates in the older age group are as high as in the general population • Rates compare to a small number of countries in Eastern and Southern Africa where surveys have been done
Prevalence rates of HIV/AIDS infection in South Africa for the age ≥ 50 years: 2005 and 2008 (percentages) Shisana et al., 2008
Respondents who underwent an HIV test in last 12 months, and received their results, South Africa 2005 and 2008
Exposure to HIV communication programmes • SA government has HIV/AIDS communication programmes and numerous NPOs implement such programmes • Communication is still poor among some high risk groups • Less than half of all adults over 50 are reached by any national programme Shisana et.al., 2008
Reach of HIV and AIDS communication by age, South Africa 2005 and 2008
Impact of HIV/AIDS on older persons HIV/AIDS impacts older persons in two ways: • Through infection: some older persons are at risk of infection with the virus, and some are already living with the disease • Through caregiving: numerous older persons care for orphaned and vulnerable grandchildren (OVC)
Older persons marginalized • HIV is viewed as disease of the young • Older persons are viewed as being sexually inactive • Their risk factors for infection are the same as in the young • HIV/AIDS is frequently misdiagnosed Older persons excluded from: • Educational programmes: • Sex education • Caregiver education
Disease burden and the older population • Older persons are at increasing risk of HIV infection • Progression to AIDS is rapid • Mortality is high due to: • Delayed diagnosis – infection not suspected • Compromised immunity that occurs with age • Presence of underlying chronic diseases, poor nutrition
Impact on older persons • Affected (indirect impact) • National level • Reduced population of working adults • Competing for fewer public resources • Physical health • Carers of sick adult children and orphans • Caregiver stress and losses • Impact on their health
Cont. • Financial • Loss of traditional support structures • An increase in medical and living expenses • Loss of wages carer may have to give up paying job • Psychosocial • Stigma: marginalized in their communities • Lack of emotional support • Pain and sadness • Fear for the future
Grandmothers supporting sick and disabled adult children and orphaned children Limited Stress Poor resources Depression health Exhaustion and increased disability Lack of support
Older people as agents of change • Older persons need basic HIV and AIDS education • Knowledge in basic nursing and parenting skills in a changing environment • Increased access to HIV and AIDS education will empower older persons to protect themselves and those in their care
Barriers to HIV/AIDS education • Majority of educators in HIV and AIDS programmes are young people • Older people are reluctant to discuss their sexuality, and personal factors affecting them and their families with young educators • Studies have shown that HIV and AIDS knowledgeable and empowered older women are effective leaders Tlou 1996 & 1997
Research Research is required to fully understand the impact of HIV/AIDS on older people and to inform the development of programmes to support them
Older persons’ contributions and needs • A Study to Understand and Foster the Functioning and Involvement of Contributive Elders (SUFFICE) is to be undertaken in Cape Town from 2010 • Will build on earlier phases of the SUFFICE pre-pilot study, completed in 2007 (Ferreira et al., 2007) • Pre-pilot study (n=55) compiled an inventory of systematic descriptions of elders who make substantial contributions to the well-being of family and community
SUFFICE Pre-pilot study demonstrated how: Health limitations impinge on elders’ capacity to contribute (more than three quarters reported a health condition), Proposed a health intervention to enhance their functioning and thereby help to preserve their contributive activities Did not specifically assess knowledge and the impact of HIV and AIDS in this population The larger planned project will contribute to development of a rationale to convince stakeholders of the merits of a health and education intervention for older people and a need to include older people in national HIV and AIDS programmes
SUFFICE 2010 • SUFFICE remains a collaborative project of institutions in Cape Town (South Africa) and New York City (USA) • The Albertina and Walter Sisulu Institute of Ageing in Africa at the University of Cape Town and the Stroud Center for Study of Quality of life at Columbia University in New York • An opportunity exists for those with common interests to collaborate in the study