Download
1 / 87
870 likes | 1.14k Views
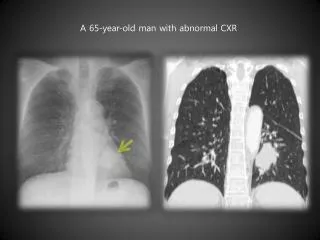
Severe headache in a 54 year-old man. Coruña | Datukon | de Castro | de la Llana April 30, 2010 | Block G NSS. CLINICAL HISTORY. General Data. I.B. 54/M Right-handed Farmer Abra. Chief Complaint. Severe headache. History of Present Illness. 1 month PTA (3/14/2010)

E N D
Severe headache in a 54 year-old man Coruña| Datukon | de Castro | de la Llana April 30, 2010 | Block G NSS
General Data • I.B. • 54/M • Right-handed • Farmer • Abra
Chief Complaint • Severe headache
History of Present Illness • 1 month PTA (3/14/2010) • (+) dizziness, (+) syncope • (+) severe headache – piercing, graded 10/10 • (+) left-sided weakness • Brought to Abra Provincial Hospital treated as a case of CVD • CT scan done in Vigan ten days post-event revealed subarachnoid hemorrhage
History of Present Illness • 1 month PTA • (-) sensorial changes • (+) minimal nape pain • (-) facial asymmetry • Advised transfer to PGH for further evaluation and surgery • Opted not to consult due to financial constraints
History of Present Illness • 2 weeks PTA • Patient was discharged asymptomatic • 1 week PTA • (+) headache - sudden onset, persistent, no noted aggravating or relieving factors, piercing, (-) radiations, graded 10/10, constant • (-) medications taken
History of Present Illness • 1 week PTA • Consulted again in Abra Provincial Hospital admitted for three days given unrecalled medications with some pain relief • Opted to take physician’s advice to seek consult in our institution
Review of Systems • (-) fever • (-) cough • (-) colds • (-) dyspnea • (-) abdominal pain • (-) bowel changes • (-) dysuria • (-) jaundice • (-) weight loss • (-) tinnitus • (-) blurring of vision • (-) rash • (-) orthopnea • (-) easy fatigability
Past Medical History • (-) HPN but with note of occasionally elevated BP on casual checking, no consults done • (-) DM, BA, PTB • (-) previous surgeries • (-) known allergies to food and medications
Family Medical History • (+) HPN – siblings • (-) DM, BA, PTB, CA • (-) CVD
Personal/Social History • (-) smoking • (-) alcoholic beverage consumption • denies illicit drug use • Married, with 3 biological children and 6 stepchildren • Farmer
Physical Examination • Conscious, coherent, not in distress • VS: BP 130/80 HR 100 RR 20 T 36.7oC • HEENT: pink conjunctivae, anictericsclerae, (-) neck vein engorgement, (-) cervical lymphadenopathy, (-) masses • Chest/Lungs: equal chest expansion, clear breath sounds, (-) rales, (-) wheezes
Physical Examination • CVS: (-) heaves, (-) thrills, distinct heart sounds, normal rate, regular rhythm, (-) murmurs • Abdomen: flat, normoactive bowel sounds, soft, nontender, (-) masses, liver edge not palpable • Extremities: pink nailbeds, (-) cyanosis, (-) edema, full & equal pulses
Neurologic Examination • Awake, coherent, oriented to three spheres • GCS 15 (E4V5M6) • Cranial Nerves I – grossly normal II, III – pupils 3mm briskly reactive to light III, IV, VI – full, equal EOMs V – intact sensation at V1-3 V, VII - brisk corneal reflexes VII – shallow R nasolabial fold
Neurologic Examination • Cranial Nerves VIII – intact gross hearing IX, X – intact gag, uvula midline XI – good shoulder shrug XII – tongue midline • Motor: good muscle tone, MMT 5/5 on all extremities
Neurologic Examination • Sensory: 100% on all extremities • DTR’s ++, (-) Babinski, (-) clonus • Meningeals: supple neck, (-) Kernig’s sign, (-) Brudzinski’s sign
Summary • 54 y/o non-hypertensive male • Apparently well until he presented with sudden-onset headache and left-sided weakness • Initially managed as a case of CVD, but with findings of subarachnoid hemorrhage on CT scan done 10 days post event
Summary • Seen in our institution 39 days post-ictus • With essentially normal physical examination findings except right central facial nerve palsy
Subarachnoid hemorrhage probably secondary to ruptured aneurysm, Grade 1
Subarachnoid hemorrhage Differential Diagnoses Diagnostics Management Outcome DISCUSSION
Subarachnoid hemorrhage • Extravasation of blood into the subarachnoid space between the pial and arachnoid membranes
Etiologies • Trauma • MOST COMMON cause of SAH • Spontaneous • Ruptured aneurysms (75-80%) • Cerebral AVMs • CNS vasculitides • Cerebral artery dissection • Coagulation disorders • Dural sinus thrombosis • No cause determined
Risk Factors • Hypertension • OCPs • Substance abuse—cigarette smoking, cocaine abuse, alcohol consumption • Diurnal variation in BP • Pregnancy and parturition • During LT or cerebral angiography in those with aneurysms • Advancing age
Cerebral Aneurysms Cerebral vsExtracranial blood vessels • Less elasticity of tunica media and adventitia • Tunica media has less muscle • Adventitia is thinner • More prominent internal elastic lamina • Subarachnoid space has very little supportive tissue
Cerebral Aneurysms • Early precursors of aneurysms are small outpouchingsthrough defects in the media of the arteries • These defects are thought to expand as a result of hydrostatic pressure from pulsatile blood flow and blood turbulence, which is greatest at the arterial bifurcations
Cerebral Aneurysms Etiologies • Congenital (Medial gap: defect in muscular layer of arterial wall) • Atherosclerotic or hypertensive • Embolic (atrialmyxoma) • Infectious (mycotic aneurysms) • Traumatic • Associated with other conditions
Cerebral Aneurysms LOCATION • Saccular aneurysms (berry aneurysms) • Located on major arteries at the apex of branch points (site of maximum hemodynamic stress on a vessel) • Fusiform aneurysms • More common in the vertebrobasilar system
Cerebral Aneurysms • Saccular aneurysms location • 85-95% in carotid system, with the ff most common locations • ACoA: 30% • P-comm: 25% • MCA: 20% • 5-15% in the posterior circulation (vertebro-basilar) • 20-30% would have multiple aneurysms
Clinical Features: Symptoms MAJOR RUPTURE IS THE MOST FREQUENT PRESENTATION • Headache • Most common, present in 97% of cases • “Worst headache of my life” • Severe and sudden • Vomiting • Syncope • Photophobia • Neck pain • Focal cranial nerve deficits (diplopia, ptosis)
Clinical Features: Signs • (+) Kernig’s or Brudzinksi’s • Coma • Increased ICP • Damage to brain tissue • Hydrocephalus • Diffuse ischemia • Seizure • Low blood flow • Ocular hemorrhage • Due to compression of the central retinal vein and the retinochoroidalanastomoses by elevated CSF pressure causing venoud HPN and disruption of retinal veins
Aneurysmal Rupture • The probability of rupture is related to the tension on the aneurysm wall • Law of La Place: tension is determined by the radius of the aneurysm and the pressure gradient across the wall of the aneurysm • The rate of rupture is directly related to the size of the aneurysm • < 5 mm: 2% risk of rupture • 6-10 mm: 40% have already ruptured upon diagnosis
Aneurysmal Rupture • Blood extravasates under arterial pressure into the subarachnoid space and quickly spreads through the CSF around the brain and spinal cord • Direct damage to local tissues • Increased ICP • Meningeal irritation
Grading SAH • Grades 1 & 2: operated ASAP as soon as an aneurysm is diagnosed • Grade > 3 managed until condition improved to grade 2 or 1 • Exception: life threatening hematoma or multiple bleeds (operated on regardless of grade)
Grading SAH MORTALITY • Admission Grade 1 or 2: 20% • OR Grade 1 or 2: 14% • Rebleed: major cause of death for Grade 1 or 2 • Signs of meningeal irritation increases surgical risk
SAH Grading • The Hunt and Hess and the WFNS grading systems correlate well with patient outcome • The Fischer classification predicts the likelihood of symptomatic cerebral vasospasm, one of the most feared complications of SAH • All 3 grading systems are useful in determining the indications for and timing of surgical management
Differential Diagnoses • Stroke • Aphasia • First Seizure in Adulthood • AVMs • Frontal Lobe Syndromes • Aseptic Meningitis • Hydrocephalus • Basilar Artery Thrombosis
Differential Diagnoses • Intracranial Hemorrhage • Cerebellar Hemorrhage • Cerebral Aneurysms • Cerebral Venous Thrombosis • Meningococcal Meningitis • Epidural Hematoma • Migraine Headache
Workup • Serum Chemistry Panel • CBC • PT PTT • Blood Typing/Screening tests • Imaging • CT without contrast is the most sensitive imaging study in subarachnoid hemorrhage.
Workup: CT Scan • Findings may be negative in 10-15% of patients with SAH • Maximum sensitivity is within 24 hours post-injury • Sensitivity is 80% at 3 days, 50% at 1 week
Workup: CT Scan • Look for evidence of hydrocephalus • trapped temporal horns and "Mickey Mouse" appearance of ventricular system • Intraparenchymal clot, intraventricular hematoma, and interhemispheric hematoma • Degree and location of SAH are significant prognostic factors.