Download

1 / 38
380 likes | 765 Views
Spina Bifida: Update 2008. Joshua J. Alexander, MD Director The Spina Bifida Clinic at UNC. Objectives. 1. Recognize the different types of Spina Bifida 2. Know why Spina Bifida happens (and how to reduce its incidence)

E N D
Spina Bifida: Update 2008 Joshua J. Alexander, MD Director The Spina Bifida Clinic at UNC
Objectives • 1. Recognize the different types of Spina Bifida • 2. Know why Spina Bifida happens (and how to reduce its incidence) • 3. Be familiar with the latest medical and surgical management options for prenatal and pediatric patients.
Outline • 1:00-1:10 Introductions • 1:10-1:20 What is Spina Bifida • 1:20-1:45 Cause and prevention • 1:45-2:15 Medical and Surgical Management options • 2:15-2:30 Questions/ share your experiences/ evaluations
Outline • Types of spina bifida • History, prevalence, incidence, etiology and prevention of spina bifida • Prenatal diagnosis and management • Motor effects • Sensory effects • Hydrocephalus and Arnold-Chiari II malformation • Spine abnormalities • Neurogenic bowel and bladder • Secondary conditions • My approach to care
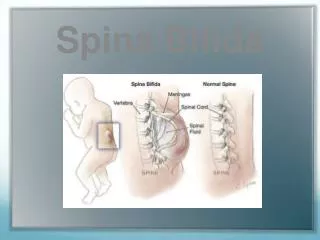
Spina Bifida Occulta • Failure of vertebrae to fuse (L-S level) • Associated spinal cord or nerve root malformations • Pigmented nevus, angioma, tuft of hair, dimple or dermal sinus • KEY RISK = tethered cord • Not usually associated with Arnold-Chiari malformation
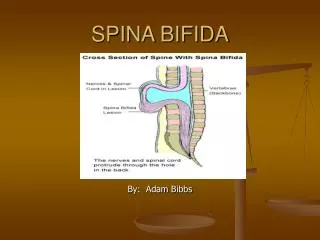
Spina Bifida Cystica • Meningocele = menigeal cyst filled with fluid. Not associated with hydrocephalus • Myelomeningocele = sac also contains dysplastic nerve tissue
History -1652 • Nicolaas Tulp, MD
History (continued) • Giovanni Morgagni (1761) • Arnold & Chiari (1890’s) • John Holter (1955) • William Sharrard (1963) • Jack Lapides (1972) • Shurtleff (1982) • Czeizel and Dundas (1992)
Prevalence • 2nd most common disability in childhood • 1/1000 live births nationally • (1-2/1000 live births in North Carolina)
Incidence • Increased risk in those of Irish, German, or Hispanic descent • In NC, Latinos are twice as likely as other groups to have a child with Spina Bifida- 2008 NC MCH report) • Decreased risk in Asians and Pacific Islanders
Why Does it Happen? • Polygenic Inheritance • Environmental Influences (Nutrition, diabetes, heat, valproic acid use) • MTHFR (?) • Folic Acid
Folic Acid • Can reduce risk of neural tube defects (including spina bifida) by 50-70% • 400 micrograms each day(multivitamin) one month prior and through 1st three months after conception • NC WCH State Performance Measure 6: Percent of women of childbearing age taking folic acid regularly. 2003 2004 2005 2006 2007 Objective (%) 50 50 50 50 50 Actual (%) 42 47 47 38 38
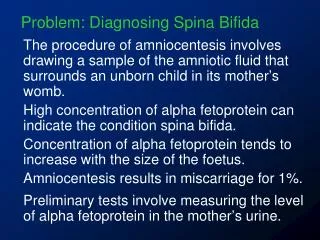
Prenatal Diagnosis • Alpha-fetoprotein in amniotic fluid (16-18 weeks) • Acetylcholinesterase in amniotic fluid • Fetal Ultrasound
Prenatal Options • Termination of pregnancy • C-section delivery • Fetal surgery
Nerve Involvement • NOT ALWAYS SYMMETRIC • Spastic and/or flaccid muscle tone • Muscle weakness • Decreased sensation • Neurogenic Bowel • Neurogenic Bladder • Vasomotor dysfunction
Motor Levels • Thoracic • L1-L2 • L3 • L4 • L5 • S1 • S2-S5
T4 T10 L1 L2 L3 L4 L5 S1 S2 S3-S5 Sensory Levels
Hydrocephalus • Most commonly due to obstruction of Cerebrospinal Fluid (CSF) Flow • VP Shunt done in 85-90% of MMC (1/3 will require revision at some time)
Hydrocephalus • Symptoms: Headache, irritability, Nausea, Vomiting • Acute Signs: Large Head, bulging anterior fontanelle, prominent scalp veins, lethargy • Chronic Signs: Decreased school performance, personality changes, decreased fine motor skills
Corpus Callosum • Connects the two sides of the brain • Commonly abnormal in spina bifida with hydrocephalus • Can be agenesis (absence) or thinning. • Can affect motor coordination, complex reasoning, problem solving
Arnold-Chiari II Malformation • Definition: Medulla, Pons, 4th ventricle +/- cerebellar vermis herniated into the cervical spinal canal • Incidence: 80-90% of those with MMC • Symptomatic: ~20%
Arnold-Chiari II Malformation • Stridor • Laryngeal nerve palsy / vocal cord paralysis • Periodic breathing • Sleep apnea • Dysphagia • Aspiration pneumonia • CENTRAL RESPIRATORY DYSFUNCTION (now the most common cause of death in MMC)
Spine Abnormalities • Bifid Spine • Vertebral fusion • Hemivertebrae
Neurogenic Bladder • Incontinence • Urinary tract infections • Hydronephrosis • Pyelonephritis • Renal Calculi INTERMITTENT CATHETERIZATION !
Mitrafanoff • Appendicovesicostomy for intermittent catheterization • Best for children with higher level lesions (less trunk control) and for girls who have hard time with cathing.
Neurogenic Bowel • Colon, Rectum and internal anal sphincter are affected • Decreased motility • Constipation • Fecal overflow • Incompetent Rectum • Fecal Incontinence and Constipation QOL NEED BOWEL TRAINING PROGRAM !
Neurogenic Bowel • High fiber diet • Stool softeners • Gastro colic reflex • Suppositories • Enemas • Biofeedback (if intact anocutaneous reflex) • MACE procedure
Fractures Charcot Joints Hip dislocation Scoliosis Kyphosis Foot anomalies Pressure ulcers Burns Obesity Precocious Puberty UTI’s Hydronephrosis Latex Allergy Syringomyelia Tethered Cord Rotator Cuff tears CTS Ulnar Neuropathy Secondary Conditions
Don’t Forget the Family !! • Family stress • Sibling stress • Divorce • Loss of family income(7-11 hours/week) • Respite • Fun !
PM&R ORTHOPEDICS NEUROSURGERY UROLOGY PT OT Child Parents Teachers Friends Nutritionist Neuropsychologist Vocational Rehab Team Approach
Crucial Periods • After diagnosis / Birth • First Year of Life • Preschool • 1st grade • Middle School • High School • Transition to Adulthood
When Should Transition Start? At Birth
How Do You Think We Can Improve Services for Children with Spina Bifida in NC?