Download
1 / 27
300 likes | 780 Views
HKCEM College Tutorial. Chickenpox. Author Dr. Shek Kam Chuen Oct 2013. Case history. F/3, come with her aunt Presented to AED for fever 38 o C & vesicular rash for one days “ ? ” cubicle nil contact, nil ILI symptom. Fever with rash. V ery S ick P eople M ust T ake N o E xercise

E N D
HKCEM College Tutorial Chickenpox Author Dr. Shek Kam Chuen Oct 2013
Case history • F/3, come with her aunt • Presented to AED for fever 38oC & vesicular rash for one days • “?” cubicle • nil contact, nil ILI symptom
Fever with rash Very Sick People Must Take No Exercise • DDX • Varicella/viral rash • Infectious mononucleosis • Dengue fever • Meningococcal disease • Drug rash, Still’s disease • Kawasaki’s syndrome: Polymorphous rash 5 Ds after fever
Diagnosis • 1. Smallpox • 2. Herpes zoster • 3. Bullous pemphigoid • 4. Bullous impetigo • 5. Chickenpox
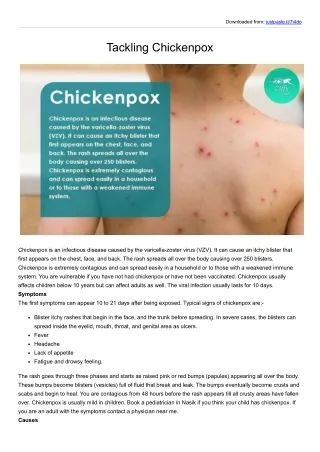
Chickenpox Rash • Initially maculopapular, then vesicles,clear fluid • Begins on face & trunk then centripetally • Vesicle are round with erythematous base • Crust • All form of lesions are concurrently present
Smallpox • Early Rash(Duration: about 4 days) • starting on the face and spreading to the arms and legs and then to the hands and feet. • Pustular Rash • BB pellets embedded in the skin • last naturally occurring case in the world was in Somalia in 1977.
Her aunt claimed that patient also pain on urination • P/E>>Vesicular Vulval Rash>>?Genital herpes • What is your action? • 1. Refer to SHS service • 2. Admit Paed as STD suspected (?abuse) • 3. Give acyclovir cream for symptomatic relief • 4. Re-assurance
Most Diagnosis are clinical • Laboratory Criteria (Any one of the following) • Isolation of varicella zoster virus (VZV) from clinical specimens • Demonstration of a ≥4x rise in antibody (Ab) titre • Demonstration of viral antigen in vescular fluid or scrapings using fluorescent-Ab staining • Positive PCR for VZV in clinical specimens HA Central Committee on Infectious Disease andEmergency Responses (CCIDER) Guideline on Varicella Zoster Virus Infections 22 May 2012
Chickenpox • Modes of transmisson: Contact, Droplets, airborne • Incubation periods: • 10-21 days • Can be prolonged to 28 days in immunocompromised patients and recipients of Varicella-Zoster IG Period of communicability: • 2 days before onset of rash and continue until all lesions are crusted • (usually within 1week from onset of rash).
You noticed • His aunt is pregnant, 35wks. • What is your action? • 1. Do nothing • 2. advice chickenpox vaccination by GP as HA will not provide chickenpox vaccination • 3. offer acyclovir PEP • 4. enquire her chickenpox status
Definition of susceptibility • Individuals are considered susceptible if they DO NOT fulfill any one of the following: • History of chickenpox/herpes zoster • History of varicella vaccination completed according to recommended schedule • Positive VZV IgG serology • Neonates (except preterm < 28 weeks or birth weight ≤1000g) born to immune mothers are protected by maternal antibody. Protection may be up to 6 months. Serological test is recommended in case of doubt
Chickenpox Status • Childhood infectious disease • >95% adult are infected in childhood • Ask patient’s mother • In case of any doubt, pls do urgent varicella IgG test. • Inform ICN to arrange an urgent test • Enter the CMS that the quarantine period • Advice patients not to attend antenatal clinic and must inform O&G MO when admitted for labour. • Arrange FU in 96 hrs
Management flowchart for susceptible pregnant women with chickenpox exposure. HKJEM 2009;01:46
Chickenpox in Pregnancy 1 • Maternal risks • In pre-antiviral era, mortality up to 25% • Chickenpox pneumonia can be up to 10% • Neonatal risks: • 2% of Congenital Varicellar Infection if < 20 weeks. • Skin contracture, scarring, limb hypoplasia • Eye, cataract • 16-29% MR, microcephaly
Chickenpox in Pregnancy 2 • Between 20 to 36 wks • No associated fetal effect • Many child present with zoster in first few year.
Chickenpox in Pregnancy 3 • > 36 weeks • Likely to infect the baby • Neonatal chickenpox
Chickenpox in Pregnancy 4 • Treatment acyclovir if within one days of rash and more than 20 weeks of gestation • Informed consent for acyclovir • VZVIG no effect if already rash develop
Chickenpox status • If IgG positive>> • If IgG intermediate>>pending confirmation test by virus unit • If IgG –ve>> • What is your action? • 1. Quarantine 10-21days after last exposure • 2. Chickenpox immunization • 3. Acyclovir daily till delivery • 4. VZVIg IMI
VZIG • Within 96hr after exposure • May prevent or attenuate infection • Limited data suggest that attenuation of disease might be achieved with VZIG up to 10 days after exposure. • Not useful if chickenpox rash already develop • Incubation period may prolong to 28 days
VZIG • IM VZIG is indicated and should be administered within 96 hours post-exposure for following high risk groups: • Immunocompromised person • Pregnant woman • Neonates whose mothers have signs and symptoms of varicella around the time of delivery (i.e., 5 days before to 2 days after). • Preterm infant <28 wk or birth weight ≤1000g exposed during neonatal period. • Preterm infant (≥28 wk) exposed during neonatal period and whose mother do not have evidence of immunity to VZV.
Other PEP to consider • VZV vaccination • As PEP within 5d of exposure for immunocompetent non-pregnant contacts >12 months of age • Acyclovir • As PEP within 10d post exposure. • No clear recommendation
Her aunt at follow up clinic • VZV IgG was +ve, now 38 week • However, she develop herpes zoster over the left chest wall. • What is your action? • Admit to isolation ward? • VZIG to mother to prevent neonatal chickenpox • VZIG to new born to prevent neonatal chickenpox • Acyclovir • Acyclovir is a FDA category B, no teratogenic effect
A 32 wks pregnant triage nurse exposed to the chickenpox • Contact tracing • no history of chickenpox • Urgent blood for IgG >> -ve • Need for PEP? • 1. VZIG • 2. Long term Acyclovir till birth • 3. Immediate immunization • 4. Is it a significant exposure?
Significant exposure • Definition of significant contact (any one): • Continuous household contact, • face to face contact > 5min, • or conversation, • Stay in the same room/cubicle for >15 min, Tang CL, et al. Hong Kong J Emerg Med. 2009;16:46-50
End THANK YOU