Download
1 / 51
550 likes | 679 Views
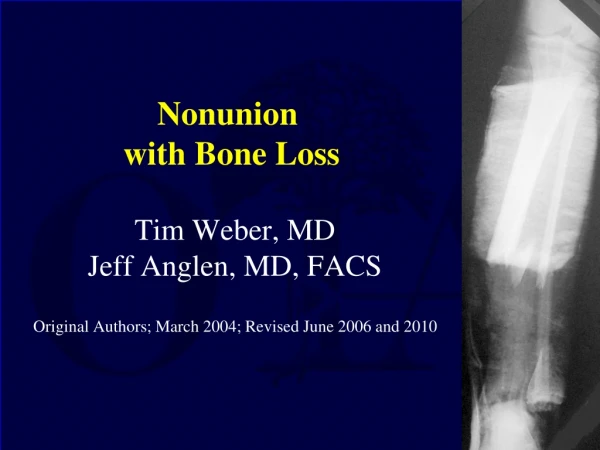
Delayed Union and Nonunion of Fractures. Amjad Moiffak Moreden, M.D. The General Assembly of Damascus Hospital Ministry of Health Damascus, Syria Feb. 28, 2006. Introduction. Approximately 5% of all long bone fractures will result in nonunions and even more in delayed unions.

E N D
Delayed Union and Nonunion of Fractures Amjad Moiffak Moreden, M.D. The General Assembly of Damascus Hospital Ministry of Health Damascus, Syria Feb. 28, 2006
Introduction Approximately 5% of all long bone fractures will result in nonunions and even more in delayed unions
Delayed Union • The exact time when a given fracture should be united cannot be defined • Union is delayed when healing has not advanced at the average rate for the location and type of fracture (Btn 3-6 mths) • Treatment usually is by an efficient cast that allows as much function as possible can be continued for 4 to 12 additional weeks
Delayed Union cont. • If still nonunited a decision should be made to treat the fracture as nonunion • External ultrasound or electrical stimulation may be considered • Surgical treatment should be carried out to remove interposed soft tissues and to oppose widely separated fragments • Iliac grafts should be used if plates and screws are placed but grafts are not usually needed when using intramedullary nailing, unless reduction is done open
Nonunion • FDA defined nonunion as “established when a minimum of 9 months has elapsed since fracture with no visible progressive signs of healing for 3 months” • Every fracture has its own timetable (ie long bone shaft fracture 6 months, femoral neck fracture 3 months)
Delayed/Nonunion Factors contributing to development: • Systemic • Local
Delayed/Nonunion cont. Systemic factors: • Metabolic • Nutritional status • General health • Activity level • Tobacco and alcohol use
Delayed/Nonunion cont. Local factors • Open • Infected • Segmental (impaired blood supply) • Comminuted • Insecurely fixed • Immobilized for an insufficient time • Treated by ill-advised open reduction • Distracted by (traction/plate and screws) • Irradiated bone • Delayed weight-bearing > 6 weeks • Soft tissue injury > method of initial treatment
Nonunion cont. Nonunited fractures form two types of pseudoarthrosis: • Hypervascular or hypertrophic • Avascular or atrophic
Nonunion cont. Hypervascular or Hypertrophic: • Elephant foot (hypertophic, rich in callus) • Horse foot (mildly hypertophic, poor in callus) • Oligotrophic (not hypertrophic, no callus) • Hypervascular nonunions. A, "Elephant foot" nonunion. B, "Horse hoof" nonunion. C, Oligotrophic nonunion (see text). (Redrawn from Weber BG, Cech O, eds: Pseudarthrosis, Bern, Switzerland, 1976, Hans Huber.)
Nonunion cont. Avascular or Atrophic • Torsion wedge (intermediate fragment) • Comminuted (necrotic intermediate fragment) • Defect (loss of fragment of the diaphysis) • Atrophic (scar tissue with no osteogenic potential is replacing the missing fragment) • Avascular nonunions. A, Torsion wedge nonunion. B, Comminuted nonunion. C, Defect nonunion. D, Atrophic nonunion (see text). (Redrawn from Weber BG, Cech O, eds: Pseudarthrosis, Bern, Switzerland, 1976, Hans Huber.)
Nonunion cont. Classification (Paley et al) • Type A<2cm of bone loss A1 (Mobile deformity) A2 (fixed deformity) A2-1 stiff w/o deformity A2-2 stiff w/ fixed deformity • Type B>2cm of bone loss B1 w/ bony defect B2 loss of bone length B3 both • A, Type A nonunions (less than 1 cm of bone loss): A1, lax (mobile); A2, stiff (nonmobile) (not shown); A2-1, no deformity; A2-2, fixed deformity. B, Type B nonunions (more than 1 cm of bone loss): B1, bony defect, no shortening; B2, shortening, no bony defect; B3, bony defect and shortening.
Nonunion cont. Treatment: • Elecrical • Electromagnatic • Ulrasound • External fixation (ie deformity, infection, bone loss) • Surgical • Hypertrophic: stable fixation of fragments • Atrophic: decortication and bone grafting • According to classification: type A : restoration of alignment, compression type B : cortical osteotomy, bone transport or lengthening
Nonunion cont. Surgical guidelines: • Good reduction • Bone grafting • Firm stabilization
Nonunion cont. Reduction of the fragments: • Extensive dissection is undesirable, leaving periosteum, callus, and fibrous tissue to preserve vascularity and stability, resecting only the scar tissue and the rounded ends of the bones • External fixator, Intramedullary nailing, Ilizarov frame
Nonunion cont. Bone Grafting origins: • Autogenous “the golden standard” • Allograft • Synthetic substitute
Nonunion cont. Bone grafting techniques: • Onlay • Dual onlay • Cancellous insert • Massive sliding graft • Whole fibular transplant • Vascularized free fibular graft • Intamedullary fibular graft
Dual onlay • Nonunion of tibial shaft treated by dual onlay grafts
Massive sliding graft Gill massive sliding graft
Whole fibular transplant Bridging of bone defect with whole fibular transplant. A, Defect in radius was caused by shotgun wound. B and C, Ten months after defect was spanned by whole fibular transplant, patient had 25% range of motion in wrist, 50% pronation and supination, and 80% use of fingers.
Vascularized free fibular graft Posteroanterior and lateral roentgenograms made 3 years after fibular transfer, showing excellent remodeling with fracture healing. (From Duffy GP, Wood MB, Rock MG, Sim FH: J Bone Joint Surg 82A:544, 2000.)
Intamedullary fibular graft Anteroposterior roentgenogram of humerus 5 months after insertion of fibular allograft and compression plating with a 4.5-mm dynamic compression plate revealing evidence of bridging callus formation and incorporation of the allograft. (From Crosby LA, Norris BL, Dao KD, McGuire MH: Am J Orthop 29:45, 2000.)
Nonunion cont. Stabilization of bone fragments: • Internal fixation (hypertrophic #): intamedullary, or plates and screws • External fixation(defects associated#): ie Ilizarov
Internal fixation Roentgenograms of patient with subtrochanteric nonunion for 22 years treated with locked second generation femoral nail. A, Preoperatively. B, Postoperatively.
Ilizarov Bifocal osteosynthesis with Ilizarov fixator after debridement of necrotic segments, as recommended by Catagni. Monofocal osteosynthesis with Ilizarov fixator for hypertrophic nonunions with minimal infection, as recommended by Catagni
Ilizarov cont. Type IIIB open tibial fracture in 30-year-old man struck by automobile. Initial treatment was with four-pin anterior half-pin external fixator that was later converted to six-pin fixator; this fixator was removed because of persistent infection. B, One year after injury, infected nonunion with deformity. C, Shape of tibial deformity is duplicated by Ilizarov frame and is gradually corrected as nonunion is compressed. D, Union obtained at 4½ months.
Nonunion cont. Factors complicating nonunion • Infection • Poor tissue quality • Short periarticular fragments • Significant deformity
Infection management Treatment of nonunion of tibia in which sequestration or gross infection is present. A, Bone is approached anteriorly and is saucerized, incision is closed, and infection is treated with antibiotics by irrigation and suction. B and C, Tibia is grafted posteriorly. B, Skin incision. C, Tibia and fibula have both been approached posterolaterally. Posterior aspect of tibia (or tibia and fibula) is roughened and grafted with autogenous iliac bone
Nonunion cont. Specific Bones Management: • Metatarsals • Tibia • Fibula • Patella • Femur • Pelvis and acetabulum • Clavicle • Humerus • Radius • Ulna
Tibia Medial Malleolus One month after intraosseous graft for nonunion of fracture of medial malleolus. B, Failure of grafting procedure. Medial malleolus was resected. C, Seven years after resection, ankle is stable, although mild arthritic changes are becoming evident. This is maximal amount of medial malleolus that can be removed if stability of ankle is to be preserved.
Tibia cont. Technique for grafting nonunion of medial malleolus
Tibia cont. Medial malleolus Sliding graft
Tibia cont. T.Shaft A, Nonunion after osteotomy. Failure to produce union by sliding inlay graft; fibula is intact. B, Four years after application of dual onlay grafts and osteotomy of fibula. Note that fibula overlaps
Tibia cont. Oblique comminuted fracture of proximal third of tibia with fracture of tibial plateau. B, Satisfactory restoration of fragments. C, Fracture of shaft failed to unite; treated by dual onlay graft.
Tibia cont. Patient with open tibial fracture treated initially with unreamed nailing. A, Broken distal screw indicated nonunion despite dynamization. B, Union achieved after exchanging nail
Femur (supracondylar) • Deformity and nonunion 7 years after supracondylar femoral fracture in 35-year-old woman; knee joint is ankylosed. B and C, Application of Ilizarov external fixator for correction of length and offset deformity. D and E, Union at 10 months.
Femoral shaft A and B, Femoral defect in 16-year-old boy; type IIIB injury was sustained in hunting accident. C and D, Six months after medullary bone graft and fixation with static-locked, unreamed, intramedullary nailing
Clavicle Hypervascular nonunion of clavicle. A, Appearance 1½ years after fracture. Nonunion painful after recent fall. B, Solid union 2½ months after compression plating and bone grafting
Humerus Combination tension band and buttress plate technique for nonunion of proximal humerus, as described by Healy, Jupiter, Kristiansen, and White. Heavy nonabsorbable suture is woven through rotator cuff using Krackow stitch and is fixed to T-plate to reduce pull of rotator cuff on proximal fragment and avoid pullout of proximal metaphyseal screws
Humerus Ununited fracture-dislocation with fracture at anatomical neck of humerus. A, Appearance on admission; four-part fracture with dislocation. B, Solid union 6 months after fixation with Neer I prosthesis. Function was satisfactory.
Humeral shaft Nonunion of middle third of humeral shaft. A, Nonunion with angulation and osteoporosis. B, Solid union 5 months after open reduction, fixation with nine-hole compression plate, and application of iliac bone grafts.
Humeral shaft Humeral nonunion. B, After fixation with intramedullary nail.
Humerus cont. Large defect in distal metaphysis of humerus after open fracture with separation of large segment of bone. B, Twenty months after bridging of defect by whole fibular transplant. Cancellous bone was used to bridge expanded portion of metaphysis and shaft.
Humeral condyle Old fracture of lateral condyle of humerus in childhood. Marked cubitus valgus and nonunion are present. B, Immediately after reconstruction. C, Twelve months later normal range of flexion and extension is restored, with normal carrying angle, 50% supination and pronation, and fair stability despite degenerative changes.
Monteggia’s Nonunion of ulna after radial head excision. Proximal ulnar fracture treated with locked forearm nail and tricortical iliac crest bone graft