Download
1 / 37
370 likes | 407 Views
Learn about pericardial diseases such as pericarditis, effusion, constrictive pericarditis, and cardiac tamponade. Discover their etiology, clinical features, diagnostic methods, and treatment options. Get insights into different types and pathologies associated with pericardial disorders.

E N D
Pericardial Diseases Prof. Lotfy Hamed Abo dahab. Professor Of Internal Medicine and Cardiology. Sohag University
Pericarditis • Etiology:. 1- Rheumatic pericarditis 2- Viral pericarditis:. - Coxsacki virus Following upper respiratory tract infection Spontaneous resolution 3- TB pericarditis 4- Pyogenic pericarditis:. - Septicemia - Pnumonia ( Staph - Strept – Pnumococci )
5- Uremic pericarditis 6- Parasitic pericarditis:. As in amoebic liver abscess 7-Traumatic pericarditis:. - In surgical operations - Motor car accidents. 8- Autoimmune diseases:. – Collagen diseases as SLE, RA – Dressler’s syndrome 9- Malignant tumours 10- Idiopathic pericarditis
Types and pathology:. 1-Dry fibrinous pericarditis 2- Pericardial effusion:. - Serous - Hemorrhagic - Pyogenic. 3- Cardiac tamponade 4- Constrictive pericarditis
Acute dry pericarditis • Clinical features:. 1- Pain:. • Common in viral cause • Uncommon in uremia and post MI. • Stabbing • Increased with respiration and movement
2-Pericardial rub:. • A scratching sound • Increases with respiration and pressure by stethoscope. • It has 3 components (atrial systole, ventricular systole, and early diastole). 3-Fever 4- Toxemia. 5- ECG:. Elevation of ST segment.
Treatment:. 1- Treatment of the cause. 2-High doses of asprine. analgesic and non-steroidal anti -inflammatory drugs. 3- Steroids and colchicine can be tried in recurrent idiopathic pericarditis.
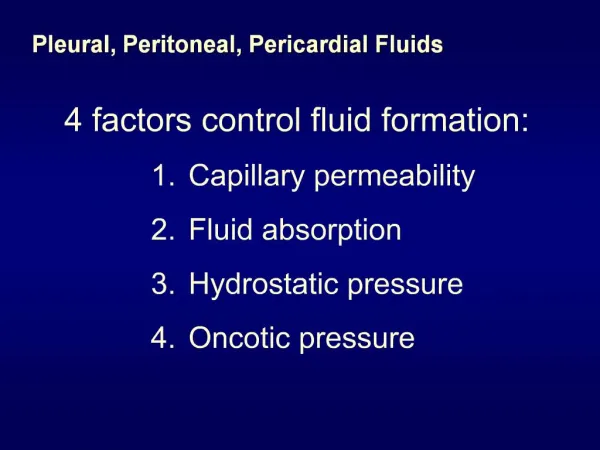
Pericardial effusion • Types:.1- Transudate:. In generalized anasarca.2- Exudate:. Follows inflammation.3- Hgic:. TB, Malignancies, trauma.4- Suppurative
Clinical features:. - The rate of accumulation of fluid determines the clinical effects of the effusion. • If massive pericardial effusion accumulates slowly, it produce no symptoms. • However, sudden accumulation of relatively small effusion may raise the intra-pericardial pressure and interfere with cardiac filling producing cardiac tamponade. Symptoms:. -Pain -Dyspnea -Compression on the surrounding structures
Signs:. Signs of effusion are difficult to detect unless nearly 500 ml fluid are present:.- Impalpable apex beat- Increase area of cardiac dullness- Faint heart sounds - Sinus tachycardia - Compression on the Lt lung may produce dullness and bronchial breathing below the inferior angle of the Lt scapula in the back (Ewart’s sign).
Investigations:. 1-X-ray chest:. - Rapid increase in cardiac shadow - Rounding in cardiac borders
2-ECG:. -Low voltage -Non-specific ST segment changes.
3-Echocardiography 4-Chemical and bacteriological examination of the fluid
Treatment:. 1-Treatment of the cause. 2-Paracentesis when there is evidence of cardiac compression. 3-Drainge in pyogenic infections
Constrictive pericarditis • Pathology:. - Healing of some types of pericarditis may result in progressive thickening, fibrosis, and fusion of the visceral with the parietal pericardium and finally calcification. - The pericardium becomes a rigid fibrous sac that constricts the heart. - The flow of blood from the atrium to the ventricle is normal in early diastole but is suddenly interrupted when the expanding ventricular wall meets the rigid pericardium
Eventually the underlying myocardium may atrophy and impaired systolic function may result. • This will result in :.-Systemic venous congestion-Reduced cardiac output • Etiology:.1- Recurrent viral, bacterial, or uremic pericarditis2- TB 3- After cardiac surgery4- Unknown
Clinical features: 1-Reduced ventricular filling :-Kussmaul’s sign , Friedieich’s sign (Raised jugular venous pressure with sharpe rise and Y descent leads to a brupt neck vein collaps ) , pulsusparadoxus 2- Systemic venous congestion 3- Pulmonary venous congestion 4- Reduced cardiac out put 5- Rapid ventricular filling (pericardial knock) 6- Atrial dilatation
Treatment: 1-Pericardiectomy 2-Treatment of the cause
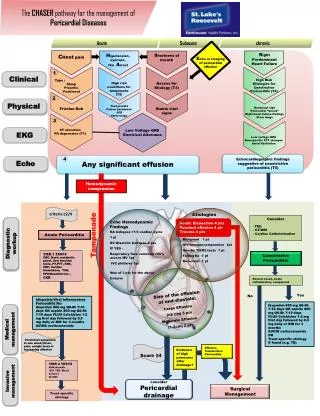
Cardiac tamponade - When the effusion worsen signs of cardiac tamponade become evident 1-Signs of systemic venous congestion. 2- Raised jugular venous pressure with sharpe rise and Y descent (Friedreich’s sign) 3- Kussmaul’s sign 4- Pulsusparadoxus 5- Reduced cardiac out put