Download
1 / 24
240 likes | 427 Views
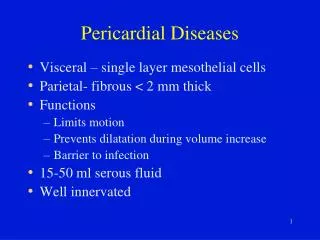
Pericardial stentless bioprosthesis. Preliminary results of a modified procedure for implantation. Y. De Bruyne, B. El Nakadi & M. Joris Hopitaux civils du CPAS de Charleroi, Belgium. 37 patients Male / female: 26/11 Age: 68 ± 6 ( 53 - 83 ) Aortic valve lesions:

E N D
Pericardial stentless bioprosthesis Preliminary results of a modified procedure for implantation Y. De Bruyne, B. El Nakadi & M. Joris Hopitaux civils du CPAS de Charleroi, Belgium.
37 patients • Male / female: 26/11 • Age: 68 ± 6 ( 53 - 83 ) • Aortic valve lesions: Stenosis: 16 (43%) Regurgitation: 10 (27%) Mixed: 11 (13%) • Endocarditis: 5 (13%)
Operative data • Size of implanted valves: • 21 mm 1 • 23 mm 7 • 25 mm 12 • 27 mm 17 • Associated procedures: • CABG 13 • Mitral repair 1
Operative groups • Group A: Classical • Classical subcoronary implantation (8/37) • Group B: Banding • Addition of peri-aortic banding (19/37) • Group C: Vascular prosthesis • Association with replacement of a dilated ascending aorta (10/37)
Group A: Classical • 8 patients • Regurgitation: 1 mild 1 severe ( reoperated ) Reconsideration of the operative technique
Implantation stentless valve dysfunction Centro-valvular regurgitation Control of sinotubular junction diameter Banding Vascular prosthesis
Implantation stentless valve dysfunction Centro-valvular regurgitation Control of sinotubular junction diameter Control of commissural alignment Banding Vascular prosthesis
Dilated aorta Non dilated aorta Vascular prosthesis Banding Group B Group C
Implantation stentless valve dysfunction Transvalvular gradient Reduction of valvular obstruction Suppression of perivalvular space Adequate scallopping GRF glue
Effect of scallopping on geometry Possibility of non cylindrical implantation Cylindrical
Implantation stentless valve dysfunction Centro-valvular regurgitation Transvalvular gradient Control of sinotubular junction diameter Control of commissural alignment Reduction of valvular obstruction Suppression of perivalvular space Banding Vascular prosthesis Adequate scallopping GRF glue
Group B: Banding (19 patients ) • S-shaped aortotomy • Aortic wall extensively freed of calcifications • Size of the prosthesis defined by the diameter of the aortic annulus • Trimming of the inferior rim of the prosthesis • Inflow suture line: 3 running sutures (Baratt-Boyes) • Scallopping of the three sinuses • Outflow suture line: 3 running sutures
Group B: Banding (19 patients ) • Dacron strip length : C = 3,5 * [prosthesis diameter] (perimeter + aortic wall thickness) • GRF Glue • Extra-aortic knots of the distal suture line anchoring the Dacron banding • Closure of the aortotomy • Fastening of the banding
Dilated ascending aorta (more than 40 mm) • Transsection at the sinotubular junction • Valve replacement (± plicatures of the aortic wall) • Vascular prosthesis (1 mm larger than the valve) • Proximal running suture supporting the valvular commissures • Distal running suture line Group C: Vascular prosthesis (10 patients )
Conclusion • The pericardial stentless bioprosthesis can be used in any pathologic condition requiering aortic valve replacement. • An appropriate peri-aortic banding seems to secure an adequate geometrical valve implantation. • Combined replacement of the aortic valve and a part of the ascending aorta seems to be a good alternative for a root replacement.
Control of sinotubular junction diameter Cylindrical configuration of the prosthesis
Control of commissural alignment Cylindrical configuration of the prosthesis
Reduction of valvular obstruction GRF glue Adequate scallopping Suppression of perivalvular space