Download
1 / 61
620 likes | 736 Views
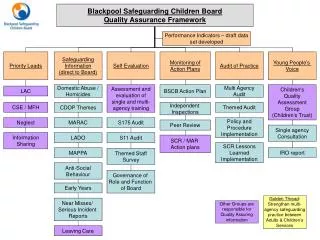
Julie Daly, Head of Service, Safeguarding and Quality Assurance Yvonne Onyeka, BSCB Business Manager. Learning from the findings of Serious Case Reviews. Objectives of the Seminar.

E N D
Julie Daly, Head of Service, Safeguarding and Quality Assurance Yvonne Onyeka, BSCB Business Manager Learning from the findings of Serious Case Reviews
Objectives of the Seminar To enable participants to reflect on the findings of Serious Case Reviews and strengthen their practice and management • Three reviews in Bromley conducted 2008 – 2010 (summaries on the BSCB website) • A briefing on the main findings of the detailed review of the findings of 268 SCRs 2007 – 2009
The Purpose of Serious Case Reviews • Public enquiries into child deaths • Chapter 8 of Working Together 2010 - when to conduct a case review - how to go about it • Learning from cases • Accountability • to the LSCB • to the community (via the local authority and other agency boards) • to central government and the general public
The Process (1) Internal agency reviews • Appoint a reviewer • Secure the written and computer records • Prepare a chronology • Interview staff • Write the agency management review • Submit the material to the safeguarding children board SCR panel
The Process (2) LSCB overview report • Appoint a SCR panel • Appoint an independent chair and report author • Produce a joint chronology • Scrutinise the individual agency reports • Evaluate the practice and agree the ‘lessons learnt’ • Write the overview report • Recommendations and an action plan
Dissemination of the findings • Feedback for staff involved • Learning for other staff and managers • Local agency boards and the council • Reports submitted to central government • Department for Education • Strategic Health Authority • Publication of the Full Report
References Brandon, Bailey & Belderson: Building on the learning from serious case reviews: a two year analysis of child protection database notifications 2007- 2009 – 268 SCRS M Brandon et al, Understanding Serious Case Reviews and their impact – A Biennial Analysis Of Serious Case Reviews 2005-7, (2009) DCSF and Families / University of East Anglia Peter Reder and Sylvia Duncan, Lost innocents – a follow up study of fatal child abuse, 1999, Brunner-Routledge An overview of 55 cases subject to serious case review and reported to government in one year Peter Reder, Sylvia Duncan, Moria Gray, and Olive Stevenson,Beyond Blame: Child Abuse Tragedies Revisited,1993, Routledge An earlier review of a less representative sample of cases M Brandon et al, Analysing child deaths and serious injury through abuse and neglect - what can we learn? A biennial analysis of SCRs 2003 – 2005, Department for Children Schools and Families, 2008.
The Review of Reviews • SCRs in England • 189 in 2003-2005 • 161 in 2005–2007 • 268 in 2007-2009 2007-2009 • 675 SINs to Ofsted • 152 (57%) died • 116 (43%) serious harmed
Some population characteristics Characteristics generally consistent over years. • Half of all SCRs are babies under 1 (importance of universal services) 45% • 23% (1-5 years) (26%) • Quarter are older children – who pose a risk to themselves &/ others and needs not recognised (25%) • Three quarters killed or harmed at home • 72% white (slight under representation) • 13% mixed parentage (slightly over represented) • 8% black / black British (slightly under represented)
Population characteristics Characteristics generally consistent over years. 2007-2009 • Under 1 year 281 (45%)* • 1-5 years 136 (22%) • 6-10 years 54 (9%) • 11-15 years 81 (13%) • 16 + 66 (11%)
Population characteristics cont. Ethnicity • White 421 (75%) • Mixed 54 (10%) • Black/Black British 54 (10%) • Asian/Asian British 27 (5%) • Other 8 (1%)
Population characteristics cont. • Male 331 (54%)* • Females 286 (46%) • Disabled 21 (8%) Incident type • Fatal 381 (62%) • Serious 237 (38%) Injury
Case characteristics Parents • Domestic Violence 34% • Mental Health 27% • Drug misuse 22% • Alcohol misuse 22% • Child of teen pregnancy 7% • Parent history of being in care 7%
Case characteristics Child More than one child abused 19% Serious iIlness 7% Drug/Alcohol misuse –child 7% Mental health problems – child 6%
Themes: Legal and care status • 16% subject to a child protection plan • 13% had been previously subject to a plan • 23% listed multiple categories of abuse (nationally only 8% of CP Plans are multiple) • 4% were accommodated under s20 • 7% subject to a care or supervision order • 5% residence order
Case characteristics Relevant Factors • Physic abuse 55% • Long standing neglect 25% • Recent neglect 18% • Sexual abuse 14% • Emotional abuse 11% • Shaken Baby Syndrome 8%
Themes: Most frequent cause of death / injury • 39% subject to physical assault • (24% head injury to baby under age one) • 16% died of neglect (fires, ingesting drugs, accidents) • 12% adolescent suicide
Children who were missing or invisible • Emotionally rejected by carers • Not spoken to or kept away from professionals • Specific vulnerability not appreciated (e.g. low birth weight, developmental delay) • Siblings of the child wrongly thought to be most at risk • Unable to speak through trauma, disability or fear So professionals need to see the child, know the child and see the world through the eyes of the child!
Chaotic, overwhelmed and unsupported families • Physically and emotionally overwhelmed • 45% had moved very frequently • Negative relationships with extended family and others such as neighbours • Deprivation and environmental dangers • Pattern of low expectations held by families and by professionals • Half in families characterised by domestic violence and almost two thirds in a family with a mental illness (past or current)
Large families & neglect • 1 in 5 reviews on families with 4 or more children. • Long standing concerns about older children not considered relevant in present time • assessment of parental capacity for change needed ‘Start again syndrome’ • Focus on individual child can be lost
Community Context • 35 aged 11+ killed /harmed in community context mainly older teenagers. • Professionals increased awareness of the harmed caused by gangs/youth violence. Some victims were siblings of gang members • Absconding (running away regularly) • Alcohol and drug excessive use • Aspects of unsatisfactory or neglectful care of a disabled child –in/formal arrangements of care
Findings from the earlier 2003 – 2007 review of SCRs • Significance of mental disorder, violence and substance misuse in the earlier sample • Cumulative risk: • 34% of cases had 3 of these risk factors • 34% had two • (so 68% had 2 or more) • 19% had one • but 13% had none at all
A hazardous and frightening home life • Substance misuse, mental ill health, domestic violence and poor living conditions • Don’t always predict serious harm but these factors hugely increase risk to children • Points to the need for a holistic assessment
The need for dynamic assessment • Stresses the importance of assessment based on ‘dynamic analysis’ as opposed to ‘description’ • Risk produced by the interaction of experience, current environment, the challenge of parenting, family and personal history and relationships • Developing and testing hypotheses about care and the child’s safety • Identifying areas where change is needed • Predicting capacity to change and care effectively • Analytical assessment leads to safer practice
Risks from organisations cont • Lack of capacity / resources was not always a feature of the review • Some individual professionals and organisations were overwhelmed by the nature and the volume of the work • Some families can drain the capacity to think and see clearly • This can contribute to lowered expectations • Refusal of some professionals to be ‘judgemental’ • Attention focused in one professional or organisational ‘silo’
Risks from organisations and professionals …. • Fixed views about the family (not responsive to signs of deterioration) • Risks associated with certain types of parenting were underestimated (e.g. ‘rough handling’) • Underestimating the need for high level support for carers - foster care mother & baby placements • A need for respectful uncertainty & dogged professional challenge
The assessment and involvement of men • Dearth of information (some organisations and professionals collude in this) • Failure to involve men in assessment • Fear of some aggressive men shaped practice • Rigid and fixed thinking – men seen as either ‘good’ or ‘bad’
Significance of supervision and management in this context Critical and challenging thinking about: • position and needs of the child • history and circumstances of the family • actions and attitudes of the worker • functioning of the professional network as a whole
Bromley SeriousCaseReviews Julie Daly Head of Safeguarding and Quality Assurance, LBB
Key facts • 3 month old Black African baby girl • 3 older half siblings were looked after by the local authority due to mother’s mental ill health • Abandoned by her mother after her mental health deteriorated seriously • Injured in the incident, but not badly
Concerns pointing to the need for review • No pre-birth assessment • Limited collaborative working between agencies and no pre-birth conference • Social care staff had not taken actions required by the procedures (and staff from other agencies had not challenged this) • An opportunity to review working relations between mental health and children’s staff
Agencies involved • Children’s Social Care Services • Bromley PCT • Bromley Hospitals • Oxleas NHS Foundation Trust • Metropolitan Police
Positive findings about practice • As far as the mother herself was concerned and taken in isolation from one another provision by midwife, health visitor and mental health services was good • Services were very responsive to ethnicity and cultural background
Key findings • Weak assessment by social care staff failed to take into account key factors • Rapid turnover of staff dealing with the case • Management input failed to identify weaknesses and prevent drift • Mother misled some professionals and facts weren’t checked
Key findings (2) • Inappropriate optimism based on mother’s current presentation • No challenge over referrals not responded to and actions not taken by other agencies • Mental health service worked from the assumption that mother would be able to care for the baby • CPA meetings did not consider the baby’s needs • Lack of curiosity about background and history • Level of interagency contact was far too low
Review of staffing and provision in social care referral service Routine joint planning between professionals and changes in the CPA approach in such cases Review and implementation of the peri-natal mental health protocol Review of joint training on mental health issues Revised procedures for use of mother and baby placements in such cases Key recommendations
Key facts • 3 month old mixed-race UK baby girl • Development impairment following head injury in 2009 while at home with her mother • Other injuries included old fractures of ribs, legs, knee cap, hand & fractures of skull • Parents both had histories of depression, mother self-harmed, father had a cognitive impairment
Concerns pointing to the need for review • Both parents received treatment for depression from same GP practice • Two notifications from police & evidence from midwives, health visitor of unstable parental relationship • Reports that mother self-harmed & expressed distress & frustration to health visitor & midwives about child’s crying • Father’s head injury impacted on his cognitive functioning • Health visitor and midwives identified poor parenting capacity
Agencies involved • Children’s Social Care Services • Bromley PCT • Metropolitan Police Service • Local Authority Adults & Community Services • Two Hospital Trusts • Ambulance Service • Voluntary Agency
Positive findings about practice • Health staff, having identified concerns, challenged the CSC manager regarding the decision not to undertake an assessment. • Evidence of good supervision in health to consider different options for taking the case forward with CSC.
Key findings (1) • Police and ACS fail to identify & share information with CSC on father’s risk to others • GPs did not share information with ante-natal services • CSC’s poor analysis of referral information leading to poor decision making. • CSC’s fail to make full use of the London Procedures & risk assessment matrix • The quality of the referral in relation to child protection
Key findings (2) • Failure to pass on information by CSC to a voluntary organisation • Pressure of workload and inexperience of staff in CSC leading to inappropriate allocations • Lack of timeliness in progressing assessments • Failure to assess and mobilise potential source of support in the extended family • Lack of any formal planning processes or meetings
Key findings (3) Themes • Weaknesses in the quality of risk assessment: • The relationship between adult and children’s services: • The experience and confidence of staff coupled with level of demand
Review the effectiveness of the multi-agency risk assessment training Continued training on domestic abuse Improved information sharing by and with police Front line staff feel able to openly discuss and escalate concerns Agencies aware of the need to make timely referrals to Police CAIC out of hours service Practice Standards Board to keep practice & information sharing between adult and children’s service under review. Review progress on the implementation of actions from previous SCRs. Key recommendations
CSC to reduce the impact of demand and workload on frontline staff & managers CSC to review effectiveness of arrangements with commissioned services to ensure they work within their remit. . Recommendations
Findings from the Bromley SCR in relation to Child D and Child B’
Key facts • Two white British boys aged 5 and 6 years old • Brought into care after one of the boys found to have injuries, said to be caused by father • Substantial contact between the boy’s family and agencies in Bromley • Continuing concerns about neglect over a period of five years