Download
1 / 118
1.19k likes | 1.27k Views
Learn about the Hepatitis A Virus, its characteristics, transmission, symptoms, diagnosis, prevention through vaccines, and global patterns of transmission. Understand the pathogenesis, immunity, and clinical features of Hepatitis A infections.

E N D
5 medically important hepatitis viruses: • 1. Hepatitis A: infectious hepatitis • 2. Hepatitis B: Serum hepatitis • 3. Non-A, Non-B: HCV • 4. Hepatitis D (delta agent/ Type D) • 5. Hepatitis E : Enteric Hepatitis • 6. Post transfusion: HGV Other viral causes: EB virus, CMV, Yellow fever, Enterovirus, Herpes virus
ViralHepatitis Enterically transmitted “Infectious” A E NANB Viralhepatitis Parenterally transmitted B D C “Serum” F, G, ? other
Hepatitis A Virus • Epidemic jaundice described by Hippocrates • Differentiated from hepatitis B in 1940s • Serologic tests developed in 1970s • Most commonly reported type of hepatitis in the United States
Hepatitis A Virus: • Picornavirus (RNA) • Humans are only natural host • Stable at low pH • Inactivated by high temperature, formalin, chlorine
HEPATITIS A VIRUS • Causes Hepatitis A infection • It is a enterovirus, family picornaviridae • Recently classified under Hepatoviruses • ss RNA • Non-enveloped • Icosahedral nucleocapsid • Replicates in the cytoplasm of the cell (Intracytoplasmic)
Also known as enterovirus 72 • It has 1 serotype • It has no antigenic relationship b/w hepatitis B or other hepatitis viruses Replication- similar to enteroviruses. Eg-polio virus.
Incubation period: Average 30 days Range 15-50 days • Jaundice by <6 yrs, <10%age group: 6-14 yrs, 40%-50% >14 yrs, 70%-80% • Complications: Fulminant hepatitis Cholestatic hepatitis Relapsing hepatitis • Chronic sequelae: None
Transmission • Close personal contact(e.g., household contact, sex contact, child day care centers) • Contaminated food, water(e.g., infected food handlers, raw shellfish) • Blood exposure (rare)(e.g., injecting drug use, transfusion)
Transmission and Epidemiology • Faeco-oral route • Reservoir :- humans • Children adolescents more commonly infected (an-icteric subclinical infection) • Adults: icteric manifestations • Virus is shed 2 weeks before & after appearance of symptoms.
Institutional outbreaks recorded. Eg- day care centres, hostels, ICU • Outbreaks directly related to sanitation. Eg- fecal contamination of drinking water, food grown in polluted water, street food. • Rarely transmitted by blood. Eg- seen rarely with haemophiliacs transfused with blood products
There is no chronic infection unlike in HBV or HCV because generally level of viremia is low. • Many people maybe infected and recovered (IgA seen in 50-70% of population) • Secondary attack rate in house hold contacts common
Global Patterns of Hepatitis A Virus Transmission Disease Peak Age Endemicity Rate of Infection Transmission Patterns High Low to Early Person to person; High childhood outbreaks uncommon Moderate High Late Person to person; childhood/ food and waterborne young adults outbreaks Low Low Young adults Person to person; food and waterborne outbreaks Very low Very low Adults Travelers; outbreaks uncommon
Pathogenesis and immunity • Virus replicates in GI tract and spread to liver hematogenously • Hepatocytes are infected but mechanism of cell damage is unclear. • Cytotoxic T-cells may damage the hepatocytes infected with virus. • If infection is cleared damage will be repaired and there is no chronic infection
Hepatitis from other virus usually indistinguishable pathologically (all look the same histo-pathologically)
Immune response • IgM is detected at the appearance of jaundice • Peaks 2-3 weeks, disappears in 3-4 months • So IgM Ab to HAV is important in diagnosis of HAV. • 1-3 weeks after the IgM appears IgG is seen. • IgG: provides life long immunity
Hepatitis A Infection Typical Serological Course Total anti-HAV Symptoms Titre ALT Fecal HAV IgM anti-HAV 4 5 6 12 24 0 1 2 3 Months after exposure
Clinical features • Incubation period (2-4 weeks) • Pre-Icteric phase: fever, nausea ,vomiting • Icteric Phase: jaundice, dark urine, pale stools, eleavtedtransaminases.
Spontaneous recovery is the rule in 2-3 weeks time • Most of the cases maybe asymptomatic (maybe solely detected on basis of IgGAb) • No chronic hepatitis or chronic carrier state • So no predisposition to hepatocellular carcinoma
Laboratory diagnosis • Biochemical investigations- LFT • Detection of anti HAV IgM, IgG: persists for decades • Detection of HAV particles: Immuno-electon microscopy (IEM) of faeces, liver, bile • HAV antigen detection: by ELISA • Isolation in cell culture possible but not routinely done • PCR: viral RNA
Hepatitis A Vaccines: • Inactivated whole virus • HAVRIX (GlaxoSmithKline) • VAQTA (Merck Vaccine Division) • Pediatric and adult formulations • Licensed for persons >2 years
Treatment and prevention • No antiviral therapy • Formaldehyde inactivated vaccine: vaccine: (virus grown in cell culture) given to children above 12 months & adults- initial dose and booster dose 6-12 months later
Live attenuated vaccine: single dose , S/c • Detection of HAV antibody prior to vaccination is cost-effective • Passive immunization with immunoglobulin (HAV Ig) for post exposure prophylaxis can prevent disease in close household contacts & travellers
Proper hygiene and superior sewage disposal, hand washing after bowel movements etc • Good sanitation help prevent (like for any food/water borne diseases) • Chlorination of water also helps.
5 medically important viruses are described as Hepatitis virus namely- • 1. Hepatitis A(HAV) • 2. Hepatitis B(HBV) • 3. Non-A, Non-B – HCV is most common • 4. Hepatitis D (delta agent or HDV) • 5. Hepatitis E(HEV) • 6. Post transfusion- HGV –causative role unknown Others can cause inflammation of the hepatocytes but not included- EB virus, CMV, Yellow fever, Enterovirus, Herpes virus
ViralHepatitis Enterically transmitted “Infectious” A E NANB Viralhepatitis Parenterally transmitted B D C “Serum” F, G, ? other
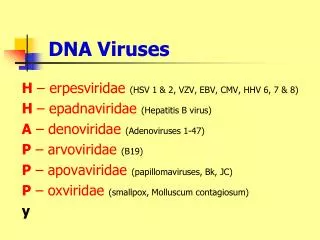
HEPATITIS B VIRUS • Causes Hepatitis B (HBV) PROPERTIES- • DNA virus, Hepadnaviridae Family • Icosahedral nucleocapsid containing partiallyds circular DNA genome.(all other Hepatitis group are RNA viruses).
Envelope contains protein surface antigen(HBsAg) • HBsAg was first discovered in serum of Australian aborigine. So it is called Australia Antigen.
MORPHOLOGY: • EM of serum from infected patients reveals 3 morphologic forms:
4 genes –S, C , P, X • S- region S- codes for major S S+pre S2- codes for M - HBsAg S+ pre S1 and S2- codes for L • C- region C - - HBcAg C+pre C - - HBeAg • P - - DNA polymerase • X - enhance HBxAg - maybe to exist as co-infection in AIDS, In chronic hepatitis, in hepato-cellular carcinoma
HBV Structure & Antigens Dane particle HBsAg = surface (coat) protein ( 4 phenotypes : adw, adr, ayw and ayr) HBcAg = inner core protein (a single serotype) HBeAg = secreted protein; function unknown
Epidemiologically: 4 serotypes of HBV (HBsAg) • ‘a’ – group specific antigen • ‘d’ or ‘y’ 2 sets of neutrally exclusive epitopes • ‘w’ or ‘r’ • adw, adr, ayw and ayr are the serotypes • ayw-West Asia, Mid-east to West & North India • adw- Europe, Australia, Americas • adr- South and East India, Far East. • ayr- very rare.
Transmission and epidemiology- 3 main modes- • Blood, blood products, IV drug abuse • Sexual contact • Perinatally from mother to new born • Very small amount of blood necessary for transmission. Eg. Needle stick injury
Concentration of Hepatitis B Virus in Various Body Fluids Low/Not High Moderate Detectable blood semen urine serum vaginal fluid feces wound exudates saliva sweat tears breastmilk
Distribution • Worldwide, particularly prevalent in the oriental countries- including India. • These areas have high incidence of hepato-cellular carcinoma- hepatoma. • HBV is a tumor associated virus • Immunization against HBV in Taiwan has decreased the incidence of hepatoma. • HBV vaccine: first vaccine against human cancer
Mutants- Few cases of Hepatitis B will be with mutant virus • Called as pre core mutants – so unable to synthesize HBcAg • Escape mutants – found in those with combined immunization- also called as ‘a’ antigen mutation. They may pose problem in prophylactic immunization.
PATHOGENESIS OF HEPATITIS B: • Why is Hep B virus specific for liver cells? • Because virus specific receptor on cell membrane facilitates entry. • Transcription factors facilitating viral mRNA synthesis.
Summary of the Replicative cycle • Viral entry- uncoating • Viral DNA polymerase synthesize missing portion of DNA • Closed dsDNA formed in nucleus of host cell • This DNA will act as template for mRNA synthesis with help of cellular mRNA polymerase • The mRNA formed functions for protein synthesis and also template for positive strand of DNA