Download
1 / 60
1.86k likes | 4.84k Views
Fertilization and implantation. Definitions. Pregnancy – events that occur from fertilization until the infant is born Conceptus – the developing offspring Gestation period – from the last menstrual period until birth Preembryo – conceptus from fertilization until it is two weeks old

E N D
Fertilization and implantation Mrs. Mahdia Samaha Kony
Definitions • Pregnancy – events that occur from fertilization until the infant is born • Conceptus – the developing offspring • Gestation period – from the last menstrual period until birth • Preembryo – conceptus from fertilization until it is two weeks old • Embryo – conceptus during the third through the eighth week • Fetus – conceptus from the ninth week through birth Mrs. Mahdia Samaha Kony
Definitions • Fuse- to physically join together • Ovum – egg cell (female gamete) • Cleavage – process of cell division during development • Differentiation – the process of forming different kinds of cells from similar cells of the early embryo • Embryo – an organism in an early stage of development Mrs. Mahdia Samaha Kony
Definitions • Fertilization or conception: Union of the sperm and ovum • A “blastocyst”: is a fluid-filled mass with an outer ring • Morula – solid ball of cells formed from cleavage • Blastula – hollow ball of cells formed from cleavage • Gastrula – a hollow ball of cells with an “in pushing” and 3 layers (germ layers) Mrs. Mahdia Samaha Kony
Relative Size of Human Conceptus Mrs. Mahdia Samaha Kony
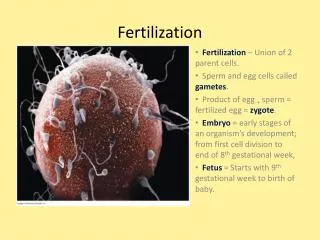
Fertilization • The oocyte is viable for 12 to 24 hours • Sperm is viable 24 to 72 hours • For fertilization to occur, coitus must occur no more than: • Three days before ovulation • 24 hours after ovulation • Fertilization – when a sperm fuses with an egg to form a zygote Mrs. Mahdia Samaha Kony
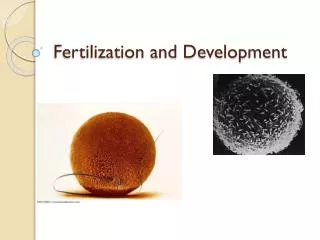
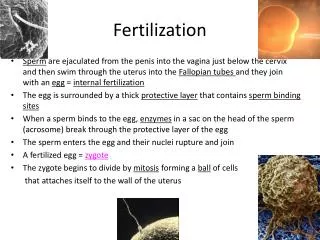
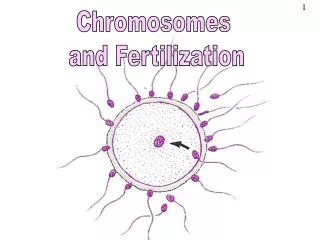
PRINCIPLES OF FERTILIZATION (CONCEPTION) • During sexual intercourse, 2 to 5 ml of semen, usually containing more than 300 million sperm, is ejaculated into the female's vagina. • The sperm make their way through the fluids of the cervical mucous, across the endometrium, and into the fallopian tube to meet the ovum in the ampulla • Only one sperm is required for actual fertilization, but the presence of many increases the chances for one to penetrate. Mrs. Mahdia Samaha Kony
Fertilization: Four Major Steps • Sperm contacts the egg • Sperm or its nucleus enters the egg • Egg becomes activated and developmentalchanges begin • Sperm and egg nuclei fuse Mrs. Mahdia Samaha Kony
Sperm Transport • Fates of ejaculated sperm • Leak out of the vagina immediately after deposition • Destroyed by the acidic vaginal environment • Fail to make it through the cervix • Dispersed in the uterine cavity or destroyed by phagocytic leukocytes • Reach the uterine tubes • Sperm must undergo capacitation before they can penetrate the oocyte Mrs. Mahdia Samaha Kony
Fertilization Mrs. Mahdia Samaha Kony
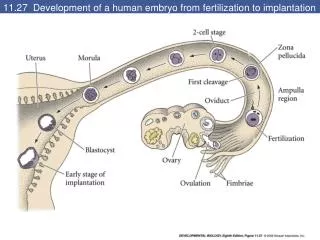
Development of the zygote • The combined ovum and sperm, referred to as the zygote, begins rapid cell division and in 2 to 3 days becomes a structure referred to as morula. • The morula is a rapidly growing structure and reaches the uterus in approximately 4 days. • The stages of development are: Fertilized ovum (zygote) 2-cell stage 4-cell stage 8-cell stage Morula Blastula Early Gastrula Late Gastrula Mrs. Mahdia Samaha Kony
Blocks to Polyspermy • Only one sperm is allowed to penetrate the oocyte • Two mechanisms ensure monospermy • Fast block to polyspermy – membrane depolarization prevents sperm from fusing with the oocyte membrane • Slow block to polyspermy : • Destroy sperm receptors • Cause sperm already bound to receptors to detach Mrs. Mahdia Samaha Kony
The Nuclei Fuse Together Mrs. Mahdia Samaha Kony
Cleavage (divide via mitosis) forms the 2 cell stage: About 24 hours after fertilization, the zygote has divided to form a 2-celled embryo Mrs. Mahdia Samaha Kony
Preembryonic Development • The first cleavage produces two daughter cells called blastomeres • Morula – the 16 or more cell stage (72 hours old) • By the fourth or fifth day the preembryo consists of 100 or so cells (blastocyst) Mrs. Mahdia Samaha Kony
They split again to form the 4 cell stage Mrs. Mahdia Samaha Kony
And again to form the 8 cell stage… Mrs. Mahdia Samaha Kony
And eventually form a Morula Mrs. Mahdia Samaha Kony
Next it becomes a blastula Mrs. Mahdia Samaha Kony
And next, a gastrula Mrs. Mahdia Samaha Kony
Preembryonic Development • A “blastocyst” : is a fluid-filled mass with an outer ring. • Inner cell mass will form the “embryo” • Outer ring—the placental/membranes • Chorionic villi from the outer ring are finger-like projections • Villi also manufacture human chorionic gonadotropin (HCG) which signal the corpus luteum within the ovaries to continue production of progesterone and estrogen to prevent menstruation. Mrs. Mahdia Samaha Kony
Cleavage: From Zygote to Blastocyst Inner cell mass Degenerating zona pellucida Blastocyst cavity Blastocyst cavity Trophoblast (b) 4-cell stage2 days (d) Early blastocyst4 days (e) Implanting blastocyst6 days (c) Morula3 days (a) Zygote(fertilized egg (a) (b) Fertilization(sperm meets egg) (c) Ovary Uterine tube (d) Oocyte(egg) Uterus Ovulation (e) Endometrium Cavity of uterus Mrs. Mahdia Samaha Kony
Implantation • Begins six to seven days after ovulation when the trophoblasts adhere to a properly prepared endometrium • The implanted blastocyst is covered over by endometrial cells • Implantation is completed by the fourteenth day after ovulation • Implantation normally occurs in the upper, posterior wall of the uterus. The point of implantation becomes the origin for the placenta and umbilical cord. Mrs. Mahdia Samaha Kony
Implantation of the Blastocyst Mrs. Mahdia Samaha Kony
Implantation of the Blastocyst Mrs. Mahdia Samaha Kony
Embryonic stage: • This stage begins at day 15 after conception and continues through week 8. • Basic structures of all major body organs and the main external features are completed during this stage. • The embryonic membranes: tow membranes form the fluid –filled amniotic sac, or bag of water, that protects the floating embryo. • Amniotic fluid: surrounds the embryo and increases in volume as the pregnancy progress, reaching approximately a litter in volume by term. Mrs. Mahdia Samaha Kony
3 weeks Mrs. Mahdia Samaha Kony
Fetal Membranes • The chorionic villi on the inner surface gradually thin and smooth out and becomes the outermost fetal membrane—the “chorionic membrane” • The second membrane is the “amniotic membrane” inner most layer. • By term, these are adherent and appear to be only one • There is nerve supply to the membranes. Mrs. Mahdia Samaha Kony
Amniotic Fluid • Clear, albuminous fluid that is 98% water. • It is constantly being formed and reabsorbed. (rate of 500ml / day) • It is never stagnant. • Fetus swallows at a rapid rate and it is a source of nutrition for the baby. • Hydramnios—excessive amounts of fluid Mrs. Mahdia Samaha Kony
Amniotic Fluid • Surrounds the embryo and increases in volume as the pregnancy progress, reaching approximately a litter in volume by term. Sources of amniotic fluid: • Fluid transported from the maternal blood across the amnion. • Fetal urine. • The amniotic fluid is changing in volume as the fetus swallow and voids. Mrs. Mahdia Samaha Kony
Functions of amniotic fluid: • Maintain constant body temperature • Permit symmetric growth and development. • Cushion the fetus from trauma. • Allow the umbilical cord to be relatively free of compression • Promote fetal movement to enhance musculoskeletal development. Mrs. Mahdia Samaha Kony
Characteristics of amniotic fluid: • It is made up of 98% water and 2% organic matter. • It is slightly alkaline • Contains albumin, urea, uric acid, creatinine, billirubin, sphygmomyeline, epithelial cells, vernix, and lanugo. Mrs. Mahdia Samaha Kony
Alterations in amniotic fluid: Oligohydramnious: deficiency in the amount of amniotic fluid<500ml at term. • It’s associated with uteroplacental insufficiency and fetal renal abnormalities. Polyhydramnious: excessive amount of amniotic fluid>2000ml at term. • It’s associated with maternal disease as D/M, neural tube defects, chromosomal deviations, malformation of the CNS, GIT malformation that prevent swallowing of the amniotic fluid swallowing. Mrs. Mahdia Samaha Kony
Placentation • Formation of the placenta from: • Embryonic trophoblastic tissues • Maternal endometrial tissues • Between the second and third month, the placenta: • Assumes the role of progesterone and estrogen production • Is providing nutrients and removing wastes Mrs. Mahdia Samaha Kony
Placentaion • The chorion develops fingerlike villi, which: • Become vascularized • Extend to the embryo as umbilical arteries and veins • Lie immersed in maternal blood • Decidua basalis – part of the endometrium that lies between the chorionic villi and the stratum basalis • Decidua capsularis – part of the endometrium surrounding the uterine cavity face of the implanted embryo • The placenta is fully formed and functional by the end of the third month Mrs. Mahdia Samaha Kony
The placenta • The placenta is the site of nutrient, gas, and waste exchange • Secretes hormones that maintain pregnancy • Trophoblast cells release human chorionic gonadotropin (hCG) which signals the corpus luteum to enlarge and produce progesterone • The placenta develops from the embryonic chorion and maternal uterine tissue • Chorionic villi are formed from the chorion, and project into the endometrium of the uterus • The umbilical cord, containing two umbilical arteries and one umbilical vein connects the embryo and the placenta Mrs. Mahdia Samaha Kony
The placenta When fully developed, the placenta serves as the interface between the mother and the fetus. Functions of the placenta: • 3 days after conception the trophoplasts secretes (hCG) which ensures the endometrium will be receptive to the implanted embryo. Mrs. Mahdia Samaha Kony
The placenta Functions of the placenta: • During the next few weeks begins to make hormones that control the basic physiology of the mother in such away that the fetus is supplied with the necessary nutrients. • It protects the fetus from immune attack by the mother. • Remove waste products from the fetus • Near the time of delivery, produces hormones that mature the fetal organs in preparation for extra uterine life. Mrs. Mahdia Samaha Kony
The placenta • At pregnancy there is no direct contact between the blood of the fetus and the maternal blood, there are always layers of fetal tissues called placental barrier. • Material can be interchanged only through diffusion. The maternal uterine arteries deliver the nutrients and the mother’s uterine veins carry oxygen and the fetal waste products away. Mrs. Mahdia Samaha Kony
Placental hormones: • Human choronic gonadotrophine ( hCG): preserve the corpus luteum and its progesterone production so that the endometrial lining of the uterus maintained , is the basis for pregnancy tests. • Human placental lactogen (hPL): modulates fetal and maternal metabolism, participates in the development of maternal breasts for lactation, and decreases maternal insulin sensitivity to increase the availability for fetal nutrition. Mrs. Mahdia Samaha Kony
Placental hormones: • Estrogen ( estriol) cause enlargement of a womans breasts, uterus, and external genitalia, stimulate myometrial contractility. • Progesterone( progestin): maintain the endometrium, decrease contractility of the uterus, stimulate maternal metabolism and breasts development, provide nourishement for the early conceptus, • Relaxine: acts with progesterone to maintain pregnancy, cause relaxation of the pelvic ligaments, softens the cervix in preparation for birth. Mrs. Mahdia Samaha Kony
Development of the Placenta Mrs. Mahdia Samaha Kony
Human Fetus at Ten Weeks Mrs. Mahdia Samaha Kony
Embryonic development: Mrs. Mahdia Samaha Kony
Origin & Development of Organs and systems • By the 16th day there are three distinct layers present called “primary germ layers” • Ectoderm—nervous system, skin, hair, nails, sense organs, mucous membranes • Endoderm—G-I tract, respiraory, lower urinary system, tonsils, thyroid, thymus glands, parathyroid • Mesoderm—supportive structures such as connective tissue, bone, cartilage, muscles upper urinary system, heart-circulatory system. Mrs. Mahdia Samaha Kony
Circulatory System • One of the first to become functional. • Heart begins to form by the 16th day. • Fetal circulation is different in that gas exchange takes place in the placenta not the fetal lungs. • Shunts are present in fetal life to accommodate these differences. • Hemoglobin has greater oxygen affinity and is more concentrated (Hgb 17.1, Hct 53 %) Mrs. Mahdia Samaha Kony