Download
1 / 32
340 likes | 664 Views
Florence ET/ECIO 2008- Terumo/Biocompatible symposium. TACE with DC beads as a pretransplant treatment for HCC Results with anatomopathological data. Pierre GOFFETTE, MD Interventional Radiology Cliniques Universitaires Saint-Luc Université catholique de Louvain Brussels.

E N D
Florence ET/ECIO 2008- Terumo/Biocompatible symposium TACE with DC beads as a pretransplant treatment for HCCResults with anatomopathological data Pierre GOFFETTE, MD Interventional Radiology CliniquesUniversitaires Saint-Luc Universitécatholique de Louvain Brussels
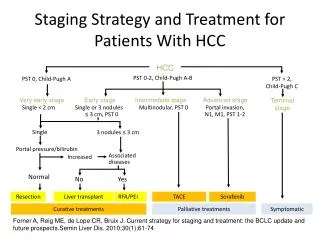
Bruix J.,Llovet J.M.: Prognostic Prediction and Treatment Strategy in Hepatocellular Carcinoma
Liver Transplantation for HCC5 year survival • Within Milan criteria>75% • Comparable to overall LT • Waiting time < 6 Mo • Drop out % 10-20% • No role for pre-LT adjuvant therapy(?) • Expandedcriteria(USCF-Mount Sinaï)25-44% (Single tum < 6.5cm or 3 tum < 4.5cm) Belghiti J. Annals Surg Oncology 2008
Liver Transplantation for HCC • Main Issues • Dropout rate 30-50% (WT > 6 Mo) • Pts beyond inclusion criteria (interm/adv) • Rationale for TACE • Bridge therapy • Control tumor + prevent progression, vasc. invasion • Neoadjuvanttherapy to improvesurvival • Downstaging(to fullfil Milan criteria) Majno P. Ann Surg 1997, Graziadei I. Liver transpl. 2003 Otto G. Liver Transpl. 2006
TACE before LTControversial Usefulness • Early stages • Effective to prevent tumoral progression • No influence on post-LT (disease-free) survival • Intermediate/Advanced stages • Effective downstaging ( > 50% red.) 35-45% • Higher post-LT recurrence rate • Lower 5 yr survival (41 vs 83%) Majno P. Ann Surg 1997, Oldhafer K. J. Hepatol 1998 , Graziadei I. L. transpl 2003, Maddala Y. L. transpl 2004, Decaens T. L. Transpl 2005 Llovet J. Sem. Liver Dis 2006, Lesurtel M. Am J Transplantation 2006
HEPATOCELLULARCATACE before LT Majno, 1999
available sizes Drug Eluting Beads (DC Beads, Biocompatible UK) RATIONALE TO USE • Delivery of large amounts of drugs to tumors for a prolonged time • Enhanced local tumor concentration • Without incresead local toxicity • Decreased serum level of chemotherapeutic agent DC Bead™ hydrogel microspheres are biocompatible, hydrophilic, non resorbable, and precisely calibrated spheres, able to load the doxorubicine. Precise and controlled release of the chemotherapeutic agent into the tumor bed.
27 patients Child-Pugh A • Response rate (CT at 6 month): 75% • Liver abscesses 2, death 1 • Median follow-up 28 months survival 1 year 92% 2 year 89% J Hepatology, 2007
Serum doxorubicin pic value (5 min) Conventional TACE : 890ng/ml Precision TACE : 90ng/ml J Hepatology, 2007
Brussels ExperienceDrug Eluting Beads for HCC before LT Single center study: 18*patients • 8within the Milan criteria • 10outside the Milan criteria • Diameter > 5cm 1 • > 3 tum < 3cm 1 • Multiple tum > 3cm8 Downstagingafter TACE ? *overall 73 HCC pts treated by DC beads over a 22 month period
Materials and MethodsHCC Characteristics • Distribution Unilobar10 Bilobar8 • Number of nodules 1(4Pts), 2(7Pts), 3(4Pts), >3(3 pts) • Size:mean5.5 cm (range 2.1-8.1) • Partial intrahepaticPV thrombosis1
Materials and MethodsDC Beads TACE protocol • Lobar(21%)-Segmental/Subsegmental(79%) injection • Standardized DC Beads doses and sizes: - 4ml (2 vials) of300-500 µmparticlesloadedwith 25mg/ml doxorubicin:100 mg Doxo/session - Dilution with 4ml of 320mg% Iodine (ratio 1/1) • Additionalunloadedparticles (300-500,500-700µ) if persitent flow • Prophylacticantibiotherapy
Materials and MethodsDC Beads TACE protocol • Sequential TACE at 3-5 Mo interval (max 4) • Alternate TACE if bi-lobar lesions • Progressive arterial feeders occlusion (3 Pts) • Tace through collaterals (phrenic, int. mam art.) • End-points Primary: Tumor response and Downstaging Secondary: HCC recurrence after LT
Procedural Results42 sessions in 18 patients • Mean number of sessions2.8 1(3pts), 2(6pts), 3(8pts), 4(1pt) • Serious adverse event2 Cholecystitis • 30-day mortality 0 • Transient impaired liver function11 No liver abcess
CT/MRI Follow-upEASL response after first TACE Complete 1(5,5%) Partial 14 (78%) Residual peripheral enhancement 7 Persistent enhanced nodules7 Stable Disease 3 Progressive disease 0 Objective response15 (83%)
CT/MRI Follow-upEASL responseafterlast TACE Complete 6(33%) Partial 10 (55%) Residualperipheralenhancement 6 Persistent enhanced nodules4 Stable Disease1 Progressive disease1 Objective response16 (89%)
First TACE session left lobe 46 yr old male: Bilobar HCC ( >7cm seg IV) Downstaging before LT
46 yr old male: Bilobar HCC ( >7cm seg IV) Downstaging before LT Repeated controls CT after first session Second TACE (right lobe) and control CT……waiting list
Patients beyond Milan criteriaDownstaging (10 Pts) • Sufficient for active LT listing 8 (80%) • Partial response 7, complete 1 • transplanted 5 • Inadequate 2 (20%) • stable disease 1 • transplanted 1 (compassionate) • progressive disease 1
66 yr old male: 6.5 cm right HCC, 1.8 cm left HCC Three selective TACE – LT 8 Mo later TACE 2 TACE 1 TACE 3
66 yr old male: 6.5 cm right HCC, 1.8 cm left HCC Three selective TACE – LT 8 Mo later
Clinical Outcome (N=18 Pts) • Transplanted patients 12 • Delay: med 8.5 Mo (3-16) • Biliary complications: 3 • Follow-up: med 8 month • 1 recurrence at 4 mo ( < 50% nec) • Patients on waiting list 5 • 1 death (pneumonia) • Drop out 1
Operative DataDrawbacks? Complicatedarterialanastomosis 7 Proper Hep. art. occlusion 4 Pedicular inflammation 3 Earlyarterial occlusion…redo-OLT in 1 Difficultbiliaryanastomosis 3 Known Doxorubicin-related complications!
Explanted SpecimenHistological data • Complete necrosis of large tumors (> 5 cm) • µ-vascular permeation in 1 patient • No inflammatory changes • Imaging for residual viable tumoral nodules • False (+) > Atypical regenerative nodule (2 Pts) • False (-) > untreated hypovascular tumor > very small viable nodules (delayed LT)
52 yr old male, ethyl cirrhosis 5.2 cm right HCC - 2 cm left HCC 3 selective TACE – LT 2 Mo later
52 yr old male, ethyl cirrhosis 5.2 cm right HCC (satellite nodules)-2 cm left HCC MRI: Partial necrosis LT: Remaining viable nodule-µvasc. permeation
Liver specimen: No viable tumoral cells 56 yr old male: 2 HCC nodules seg III-IV Three TACE
CONCLUSIONS Higher anti-tumoral response % if compared with conventional TACE Complete necrosis could be achieved even in large HCC TACE-related surgical complications mainly due to Doxorubicin Effective downstatging of most patients with intermediate-advanced HCC TACE with DCbeads could reduce the dropout % Large prospective studies are needed
Drug Eluting Beads vs Microspheres before LTNicolini A.F. March 2008-SIR Annual meeting