Download
1 / 18
190 likes | 613 Views
Scottish Cerebral Palsy Hip Surveillance Project…….First Steps. Hip Surveillance -The Swedish Experience CPUP www.cpup.se. CPUP – A preventive follow-up programme for children with cerebral palsy or suspected cerebral palsy.

E N D
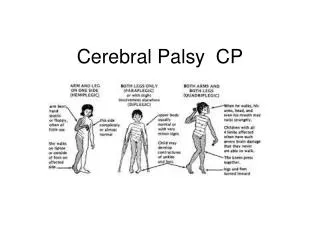
Scottish Cerebral Palsy Hip Surveillance Project…….First Steps
Hip Surveillance -The Swedish Experience CPUP www.cpup.se CPUP – A preventive follow-up programme for children with cerebral palsy or suspected cerebral palsy. • The purpose of CPUP is to ensure that children, with risk of developing significant contractures or hip dislocation are detected early and receive treatment as early as possible. • The goal is that no child should be affected by severe contractures or hip dislocation and that every child should achieve the best function possible
Hip Surveillance -The Swedish Experience CPUP www.cpup.se • The programme has been developed in collaboration with local multi-disciplinary team members such as neuropediatricians, physiotherapists, occupational therapists and orthotists and all interventions have the support of both the local team as well as the orthopaedic and hand surgeons.
Hip Surveillance -The Swedish Experience CPUP www.cpup.se CPUP – the follow up • Child’s physiotherapist and occupational therapist performs assessment of muscle tone, joint motion ability and function • twice a year until the child is aged six. • an annual assessment until the child reaches adulthood. • Current treatment described
Hip Surveillance -The Swedish Experience CPUP www.cpup.se • General recommendation radiographic examination of the hips annually from the age of two • a spinal radiograph is taken on older children and youths developing clinical scoliosis.
Hip Surveillance -The Swedish Experience CPUP www.cpup.se • All the information from the CPUP assessments is stored in a database. • a CPUP report, showing the child’s development over time and give warning signals for need for intervention. • This is fundamental in order to initiate the right treatment at the right time for each individual child.
CPUP- the results • Before CPUP, 10% of the children developed hip dislocation
CPUP – the results Contractures. The number of children with severe contractures has been reduced with 70%. The number of children with windswept deformity has been reduced, as well as the severity of the deformity
CPUP – the results The number of children with severe scoliosis has been reduced 60%.
Conclusion With a cerebral palsy register, identifying all children with CP in a population, in combination with a screening programme it seems possible to prevent or reduce the development of severe contractures, hip dislocation and scoliosis in children with CP.References1. Hägglund G, Andersson S, Düppe H, Lauge-Pedersen H, Nordmark E, Westbom L. Prevention of dislocation of the hip in children with cerebral palsy. The first ten years of a population-based prevention programme. J Bone Joint Surg 2005; 87-B:95-101.2. Hägglund G, Andersson S, Düppe H, Lauge-Pedersen H, Nordmark E, Westbom L. Prevention of severe contractures might replace multilevel surgery in cerebral palsy: results of a population-based health care programme and new techniques to reduce spasticity. J Pediatr Orthop B. 2005; 14:268-72.3. Persson-Bunke M, Hägglund G, Lauge-Pedersen H. Windswept hip deformity in children with cerebral palsy. J Pediatr Orthop B. 2006; 15:335-8.4. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997; 39:214-223.5. Eliasson A-C, Krumlinde-Sundholm L, Rösblad B, Beckung E, Arner M, Öhrvall A-M, Rosenbaum P. The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol 2006; 48: 549-554.
Range of motion measures In CPUP, use of limit values – traffic lights • Green indicates a normal or almost normal value. • Yellow : need for review of the child's present treatment. • Red value is clearly pathological.
Clinical Measures- GG&C SEMLS pathway Example Hip Abduction in ExtensionSlow passive movement R2 GMFCS I -III <30º >30º <40º >40º • Green indicates what we regard as a normal or almost normal value, • Yellow value should prompt a review of the child’s management strategy, • Red value requires referral to orthopaedic department for further assessment.
Children’s orthopaedic surgeons from the four teaching hospital centres in Scotland • Proposal to develop a screening programme for hips in children with CP. • recognised that having a broader database of relevance to physiotherapists would be an enhancement.
October ‘11 meeting with physiotherapy representatives from several Scottish regions to discuss: • the desirability of having a common proforma for children with CP • the content of such a proforma • the implications of training required for physiotherapists to use a standard proforma
Areas represented • NHSG Aberdeen • NHS Lothian. • NHS Grampian, Moray • NHS Tayside • NHSGG&C Glasgow • NHS Lanarkshire • NHS Fife • NHS Ayrshire & Arran • NHS Forth Valley • AHP National lead, CYP
Core orthopaedic clinical surveillance Proposed content • Dominant Neurological condition • Range of Motion measures for GMFCS I- III & IV-V • Spasticity reducing treatments: Botulinum toxin SDR ITB Oral antispasmodics • Hip radiographs • Orthopaedic interventions
There was agreement that the knowledge and skills required to develop the surveillance programme and carry out the required measures were integral to physiotherapy practice – The skills required were “our core business” • There would be a need to standardise the measures used and ensure consistency with clinical assessments, resulting in a training need for contributing physiotherapists
Next Steps…… • Further meetings to agree content of pro-forma • Consider local arrangements for implementing hip surveillance programme • Application for CHPO grant to support web-based education resource and training events • Develop central database