Download
1 / 49
490 likes | 510 Views
Explore the epidemiology, costs, and factors influencing morbidity in chronic back pain. Learn about diagnosis, imaging, and treatment options alongside real-life case examples.

E N D
Oh My Aching Back Deborah Van Dommelen, MD/MPH Northwestern Mutual
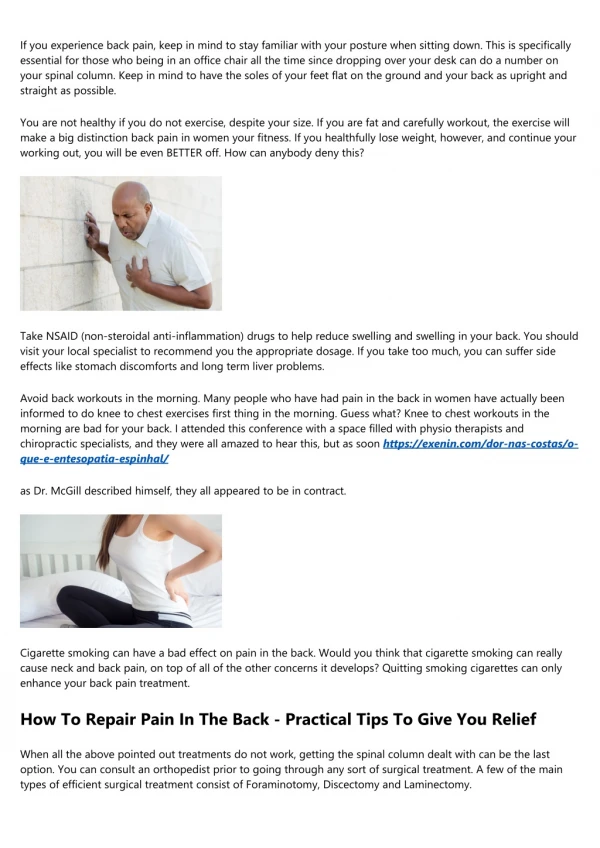
Epidemiology of Back Pain • Second most prevalent neurologic condition in the US (#1 for men) • Second most common symptom that prompts MD visit in the US • Typical age of onset is 30-50, but affects some people into later years • 80% of US population will have “disabling” back pain in their lifetime YOU WILL SEE THIS A LOT
Diagnosis Frequency by Age Age 45-64 Age >65 • Hypertension • URI • Diabetes • LBP • Hypertension • COPD • CAD • URI • Diabetes • Arthritis • LBP
Annual Costs of Low Back Pain • $40 Billion in Direct Costs • >$100 Billion in Indirect Coasts • Rapid increase in technology for imaging and procedures is a significant contributor • Of those with back pain, 75% sought medical evaluation and 25% had a related hospitalization • LTC Claims coverage could be part of these costs
Causes of Low Back Pain (LBP) • Mechanical (97%) • Spinal Stenosis • Degenerative Disc • Visceral (2%) • Aortic Aneurysm • Kidney Disease • Cancer (1%), increases with age up to 7%
Mechanical LBP • Herniated Disc • Compression Fracture • Spinal Stenosis • Ankylosing Spondylitis • Cauda Equina Syndrome • Nonspecific LBP (85%)
Spinal Stenosis • More common in men • More common in older ages • Postural versus Ischemic
Factors Determining Morbidity Risk • Duration of Symptoms (acute vs. chronic) • Recurrence • Level of Function • Imaging and Other Testing (EMG, ABI, etc) • Treatment • Medications • Procedures • Therapies
Factors Determining Morbidity Risk • Duration of Symptoms (pain)
Chronicity of Back Pain • Acute (< 6 weeks) • Lumbar Strain/Sprain • Osteoporotic Fracture • Traumatic • Subacute/Chronic (6-12 weeks/>12 weeks) • Degenerative Disc Disease • Degenerative Joint Disease • Fibromyalgia • Polymyalgia Rheumatica • Parkinsons • Lumbar Stenosis
Chronic LBP • Prior studies reported 90% of back pain resolved within 4 weeks • Recent research indicates that 62% still have back pain after 12 months • Over age 70, severity and duration of pain are strongest predictors of function and disability.
Factors Determining Morbidity Risk • Duration of Symptoms (pain) • Recurrence
Recurrence • Single Episode • Recurrent Symptoms • Asymptomatic Periods • Recurrence rate in 60-80% within 2 years • Persistent Symptoms • Never resolves • Stability • Effect on current activities (does it correlate with severity?)
Case Example #1 • 57yo female 5’ 6” 140# (22.5). Works FT. NT • Horse injury 2 yrs ago with period of paralysis (spinal cord bruising). • Neurosurgeon- Immediate quadraparesis after fall on neck. • Imaging- Vertebral fracture and cord edema. Mod stenosis multiple levels of cervical spine. • Comorbids- Osteopenia (fractured wrist due to fall off horse) • Function- Back to work within 2 months. No sx’s while taking Neurontin. Currently pain free with daily workouts. • Meds- Neurontin (weaned off within 6 months)
Factors Determining Morbidity Risk • Duration of Symptoms (pain) • Recurrence • Level of Function
Function • Unfavorable- General aging effects on the ability to compensate for pain (physiology) • Fall risk • Cognition • Tolerance of pain meds • Ability to participate in therapy • Favorable- Underwrite the specifics of this applicant • Golfing daily • Still working
The Back Pain Function Scale (BPFS) (Stratford et al) • Able to do usual work housework? • What are usual hobbies recreational or sporting activities? • Is sleep disturbed by pain? • Able to do the following for 1 hour: lifting, standing, walking, sitting, and driving? • Able to go up or down 2 flights of stairs? • Any problems putting on socks or shoes? • Working outside home? FT?
Case Example #2 • 60yo male 6’ 1” 210 (BMI 28). Works FT. • Intermittent back pain for more than 10 years. • Imaging- x-ray from 8 years ago showing mild scoliosis. • Tx includes: chiro, PT, and NSAID’s for flares. No surgeries or injections. No narcotics due to nausea. • Recurrence averages 2-3 times a year. Usually due to lifting activities related to home improvement projects. Takes 3-7 days before back to normal activities. • Most recent exacerbation 2 months ago after laying sod on 1/2 acre lot. Now reported to be sx free (completed 4 weeks of chiro). • Since then had a GXT as part of application for life insurance (13 minutes, 14 METS)
Factors Determining Morbidity Risk • Duration of Symptoms (pain) • Time to Recovery (function) • Recurrence • Level of Function • Imaging and Other Testing (EMG, ABI, etc)
Testing • Imaging • X-Rays (radiation exposure) • CT Scan • MRI • Nerve Conduction Studies (EMG) • Ankle Brachial Indices (ABI) • Bone Mineral Density (BMD)
Why so much Imaging?? • Between 1994 and 2005, Lumbar MRI’s increased by 400% in the Medicare population • Use of imaging directly affected patient satisfaction scores for providers • Scanners are more available • Medicare reimbursement much higher for MRI than traditional films • Defensive medicine (more cancer in older population)
Imaging of the Spine • Probability of identifying specific cause of back pain on radiographs < 1%. • Age contributes to false-positive findings on radiographic studies • 50% of asymptomatic people over age 40 will have an abnormal CT or MRI • Gets worse with age *Do NOT read too much into imaging*
Asymptomatic at Age 60 • Herniated Disc • Spinal Stenosis • Degenerative/Bulging Disc 36% 21% 90%
Does Imaging Mean Anything? • Does the location of symptoms match the abnormality on CT/MRI? • Is the severity of symptoms consistent with the degree of abnormality on the CT/MRI?
Case Example #3 • 57yo male 5’ 9” 195# (BMI 29) • No prescription meds. PRN OTC NSAID. • End stage DDD. Imaging from 2006 shows loss if disc space at L4-5 with impingement of L5 nerve root. Disc extrusion affecting L3 and L4 nerves. • Neck pain in 2009 treated with chiro, then 2 prednisone bursts, followed by an epidural
Case #3 continued • Works 50 hours a week as an executive and volunteers in his free time. • Prior disc surgeries in 1980’s. No issues since then. No current symptoms. • Appears agile on exam with no gait abnormalities. Able to rise out of chair without assist.
Treatment • Chiropractic Adjustments • Adaptive Devices • Epidural Injections • Nerve Stimulation (TENS) • High Risk Medications • Surgery
Beers Criteria • Potentially “inappropriate” medications for older adults (65+). • Higher risk for toxicity • Higher risk for side-effects • Generally ineffective • For full list of medications, refer to this site: http://archinte.ama-assn.org/cgi/content/full/163/22/2716
Beers Criteria (LBP related) • Any benzodiazepine (alprazolam, lorazepam, etc) • Muscle relaxants (Soma, Paraflex, Skelaxin, Flexeril, etc) • Anti-inflammatory (Toradol, Indocin, Naprosyn, Daypro, etc) • Narcotics (Demerol) • Miscellaneous (Elavil) • NO MORE Darvocet
So what medications are left for pain management? • Tylenol • Narcotics • Oral vs. parenteral/patch/cocktail • Potency • Scheduled vs. intermittent use • Neurotin/Lyrica
Surgical Outcomes • Discectomy improvement demonstrated at 1 year, but not at 4 years or 10 years. • 70% will develop recurrent back pain years later • Risk of disc herniation is 10X higher in this population What is underlying anatomic abnormality that allowed the initial lesion?
Case Example #4 • 55yo female 5’ 7” 210# (BMI 33). Works FT. NT. • PMH- Osteopenia, hypothyroid, lumbar fusion (15yrs ago). • Recent visit- Left LE numbness associated with chronic LBP and radiculopathy (occasional weakness). Has cane and walker at home but does not use them. • Treatment- Prior back surgery failed (remote). Radiofrequency ablation little improvement. ESI last month.
Case Example #4 Continued • Comorbids- Osteopenia treated with fosamax, but stopped due to GI sx’s. No follow-up BMD. • Meds- tried neurotin and lyrica (too sedating). GI upset with NSAID’s. So given narcotics and steroid bursts for exacerbations. • Imaging- Mod degenerative changes lumbar and cervical spine (osteophytes and disc space narrowing). Noted hardware for prior fusion causes artifact)
Take Home Pearls…………………… • Is this really Mechanical back pain? • Is my decision overly influenced by Imaging? • Does Treatment match the symptoms? • Are there any Co-morbid conditions to be considered? • What is their Function?