Download
1 / 52
1.16k likes | 3.59k Views
CARCINOMA STOMACH . PROF.DR.V.SHRUTHI KAMAL. INCIDENCE. GLOBAL STATISTICS 640600 MEN 349000 WOMEN 50% adavanced carcinoma CA CANCER J.CLIN 2011 . Distal cancer Increase in proximal cancers Incidence remains high in Japan

E N D
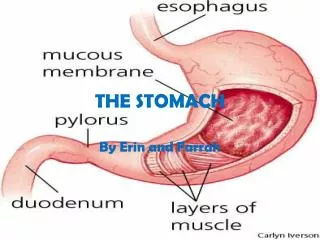
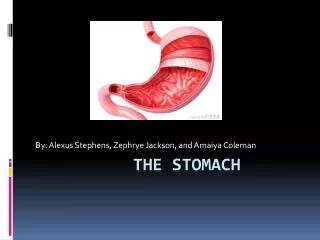
CARCINOMA STOMACH PROF.DR.V.SHRUTHI KAMAL
INCIDENCE • GLOBAL STATISTICS 640600 MEN 349000 WOMEN • 50% adavanced carcinoma • CA CANCER J.CLIN 2011
Distal cancer • Increase in proximal cancers • Incidence remains high in Japan • Their cure rates better due to screening/ survellance/early detection
Age • Average age of onset 55 yrs
Etiology • Diffuse cancer Proximal & hereditary • Intestinal type Distal cancers younger Endemic/ inflammatory changes with Helicobacter pylori infection
DIET • Linked to High ingestion of Redmeat/cabbage/spices/fish/smoked Salt preserved/high carohydrates • Low ingestion of fruits vegetables Fat /protein/vitamins A,C,E
Gastric Cancer – Dietary/Lifestyle Factors Carl-McGrath S, et al. Cancer Therapy (2007).
Helicobacter pylori infection • Increased risk • HP organism found in 89% intestinal type/32% with diffuse type • Trials in eradicating HP infection
Heredity & Race • African/Asian/Hispanic American >risk • Whites< risk
Anemia –pernicious anemia • 3to18 times > risk • Achlorhydria • Atrophic gastritis
Previous Gastric resection • Gastric stump ca > 15 to 20 yrs • Alakaline bile/dysplasia of gastric ca/ elevated gastrin levels > carry poor prognosis
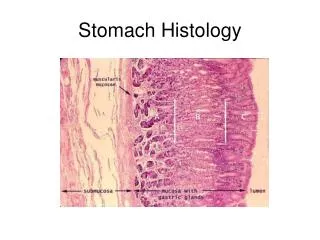
Mucosal dysplasia • Grade I to III • High grade dysplasia >marker for future gas .ca • Intestinal metaplasia/ replacement of • Glandular epithelium> intestinal type
Gastric Cancer – “Correa Sequence”- pathophysiology Potentially reversible “Vogelgram” of CRC Not HGD Chronic gastritis Mucosal atrophy Intestinal metaplasia Intestinal-type carcinoma Normal Dysplasia Increasing risk http://www.hopkinscoloncancercenter.org Hartgrink HH, et al. Lancet (2009).
Gastric polyps • FAP ( Familial adenomatouspolyposis) • Have > incidence of gas .ca/advised endoscopy/ survellence • Hyper plastic>do not have malig.potential
Chronic gastritis • Atrophic gastritis( autoimmune) • Hypertrophic gastritis Menetriers
Other risk factors • > 50 yrs • Blood group A • Lower socio economic status • Alcohol • Smoking • Obesity
Histology • Adeno ca >95% • Leiomyo sarcoma • Lymphomas • Squamous ca >5% • Carcinoid
Other risk factors contd E cadheringene mutation HNPCC LIFraumen EB virus
Pathology • Gross types> cauliflower ulcerative Leather botttle (linitisplastica)
Lauren’s • Intestinal type(53%) Good prognosis HP infection • Diffuse type(33%) Bld group A,Familial, signet ring,poor differentiation , younger bad prognosis
Japanese classification • Early gastric > mucosa+ submucosa+ or - nodes • 1 protruded cure rate >95% • 2 superdicial • 3 Excavated
Advanced gastric ca • Muscularis+serosa + or – nodes • Borrman’s classification • I single polypoid • II ulcerated ca + clear margin • III ,, ,, ,, + with out clear margin • IV diffuse & V unclassified
MINGS classification • Expanding • Infiltrative
WHO Histological( Microscopic) • Adeno ca>papillary,tubular mucinous ,signet Adenosuamous Squamous undifferentited
Siewertclassifiaction • Proximal gas .ca • TypeI Ca of GE ( Barrets) • TypeII With in 2 cmsSquamo columnar junc • TypeIIISubcardial
Location of cancers • Distal >40% • Proximal>35% • Body>25%
Spread • Local Ulcerative> gsatric wall> serosa • schirrous>submucosa/muscularis • Lymphatic • Virchows node ( left supraclavicular ) • Left axillary (Irish node) • Blood spread>liver 40%Lung 40% • Sclerotic bone mets/carcinomatous meningitis
contd • Peritoneum 10% seedling of peritoneal surfaces • Umbilicus/falciform(sis Mary joseph nodule) • Krukenberg>mets to ovary • Blumer shelf ( rectal shelf in men)
Paraneoplastic syndrome • Polymyosistis • Dementia • Venous thrombosis • Ectopic cushing • LeserTrelatsign( seborheickeratosis) • Acanthosis
Diagnosis • Anorexia/early satiety/dyspepsia • Dyspagia/weakness/ • Abdominal pain>60% • Weight loss>50% • Nausea vomiting>40% • Palpable mass>30% • Haemetemis/ malena>25%
Investigations • CBC/LFT/Chest x-ray • EGD( esophagogastroduodenoscopy) • USG/EUS(endo ultrasound) • CT • Diagnostic lap
Staging • TNM Tx cant be assessed • T0 No eveidence of tumour • Tis in situ • T1 lamina propria or submucosa • T2 a –muscularispropria • T2 b—invades subserosa • T3 invades serosa T4 adjacent structure
Gastric Cancer – Staging Systems • TNM: most important clinical prognostic factor http://www.hopkins-gi.org http://www.medscape.com/viewarticle/543068_3
Nodes • Nx cant be assessed • No no nodes • N1 1-6 nodes • N2 7-15 nodes • N3 > 15 nodes
Meatastasis • Mx Mets cant be assessed • Mo No mets • M1 distant mets
Management • Surgery > Curative • 1 Endoscopic mucosal resection • 2 Subtotal gastrectomy distal 2cm & proximal 5 cm clearance(Billroth II) • 3 Total gastrectomy (Roux en y)
Inoperable tumours • Multiple mets liver • Extensive invovolment adjacent organs • SMV/SMA • Carcinomatosisperitonei
Resection • R0 resection > No residual disease • R1 >microscopic residual disease • R2> Macroscopic residual disease • R3> unresectable
Nodal stations • First tier nodes 1-6 nodes • Second tier nodes 7-11 nodes • Third tier nodes 12-18 nodes • D1 dissection nodes are N0 (3-6) • D2 dissection(N1) 1-11 removed • D3dissection(N2)paraaortichepatodudenal D4 1-18 stations
Surgery -contd Palliation • Palliative resection • Palliative by pass Anterior Gastrojejunostomy/feeding jejunostomy • Laser ablation/ stenting • Pain relief
Chemotherapy Adjuvant chemo therapy 5 FU225mg/m2/days 1-5/1-21 Epirubicin50mg/m2 day1 Cisplatin60mg/m2/day1
Chemo for advanced ca • ECF epirubicin/5 FU/Doxorubicin • EOX epirubicin/0xaliplatin/capecitabine • DCF Docetaxel/cisplatin/5FU
Radio therapy-Role • Helpful in palliation for unrsectable tumors(4000cgy 4wks) • IORT (tumour bed)
Prognosis • Early 5 yr survival 70- 90% • Advanced ca less than 20% • Recurrence with in 3 yrs
Gastric lymphoma • Primary- elderly/NHL-B cell type • Mucosal associated lymphoid tissue (MALTOMA)/H.pylori Loss of appetite/pain abdomen/wt loss Mass abdomen Associated SLE/HIV/Ch gastritis etc
complications • Obstruction • Perforation • Bleeding • metastasis
treatment • Treat HP infection • Surgery for obstruction • Chemo same as NHL
GIST-gastroinestinalstromal tumor • Non epithelial /equal sex incidence • 50-70 yrs • Arises from interstitial cell of cajal • Treat surgery • Chemo sunitinib • imatinib