Download
1 / 56
570 likes | 640 Views
Explore the structure and functions of the stomach, including vascular supply, lymphatic drainage, tissue layers, microscopic anatomy, and cellular components. Understand how the stomach's specialized epithelial cells work to protect against harmful substances.

E N D
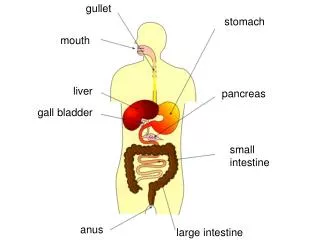
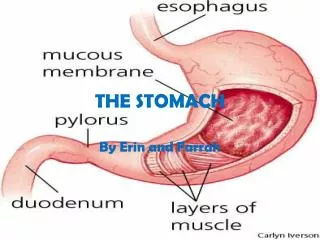
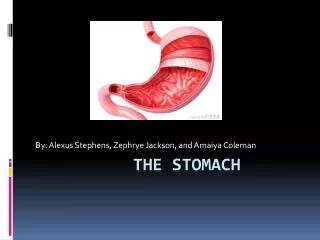
Stomach: a J-shaped dilation of the alimentary canal with the esophagus proximally and the duodenum distally • EG Junction, Fundus, Cardia, Body, Incisura, Pylorus • Functions: primarily as a reservoir to store large quantities of recently ingested food, thus allowing intermittent feedings, initiating the digestive process, and releasing its contents in a controlled fashion downstream to accommodate the much smaller capacity of the duodenum • The stomach volume ranges from about 30 mL in a neonate to 1.5 to 2 L in adulthood
Vascular • Vascular: Arteries • Lesser: Celiac… common hepatic…. left and right gastric artery • Greater: Splenic… left gastroepiploic & Gastroduodenal….right gastroepiploic • Fundus & left upper view of greater curvature… Short gastric • Venus drainage: • compatible with arteries… drain to Portal vein • Lesser: right & left gastric vein…PV • Greater: Inf: left & right gastroepiploic… gastrocolic …. SMV…PV • Sup: Short gastric….splenic vein… SMV ….PV
Lymphatic • Lymphatic: drain to celiac nodes • Inferior gastric to subpyloric &omental nodes….Hepatic nodes….Celiac • Greater curvature….Pancreaticosplenic nodes…. Celiac • Lesser(superior gastric) …. Left & right gastric…. Celiac • Pyloric portion…. Suprapubic nodes… hepatic ….celiac • Innervation:Sympathetic • Preganglionic fibers(T6 to T8 spinal nerve)…. Bilateral synapses with Celiac ganglion …. Celiac plexus(post ganglionic fibers) ….. Pain & motor fiber to pyloric sphincter • Parasympathetic: Right & left vagus(Distal esophageal plexus) ….. Posterior & anterior vagal trunks(post. & anter. Stomach)
TISSUE LAYERS OF THE STOMACH • The luminal surface of the gastric wall forms thick, longitudinally oriented folds, or rugae • Four layers make up the gastric wall: mucosa, submucosa, muscularis propria and serosa • Mucosa lines the gastric lumen, appearing as a smooth, velvety, blood-filled lining • The mucosa of the cardia, antrum, and pylorus is somewhat paler than that of the fundus and body(functional secretory elements) • The submucosa, immediately deep to the mucosa, provides the dense connective tissue skeleton of collagen and elastin fibers • Lymphocytes, plasma cells, arterioles, venules, lymphatics, and the submucosal plexus are also contained within the submucosa.
TISSUE LAYERS OF THE STOMACH • The third tissue layer, the muscularis propria, is a combination of 3 muscle layers: inner oblique, middle circular, and outer longitudinal • The inner oblique muscle fibers course over the gastric fundus, covering the anterior and posterior aspects of the stomach wall • The middle circular fibers encircle the body of the stomach, thickening distally to become the pyloric Sphincter • The outer longitudinal muscle fibers course primarily along the greater and lesser curvatures of the stomach • The final layer of the stomach is the transparent serosa, a continuation of the visceral peritoneum
MICROSCOPIC ANATOMY • The gastric mucosal surface is composed primarily of a simple layer of columnar epithelial cells 20 to 40 μm in height • These surface mucous cells which are similar throughout the stomach, contain basally located nuclei, prominent Golgi stacks, and dense cytoplasm with especially apically located, dense, mucin-containing membrane-bound granules • The cells secrete mucus in granules that are released via exocytosis, apical expulsion, and cell exfoliation • The primary role of mucus, along with bicarbonate, is luminal cytoprotection from “the elements”: acid, pepsin, ingested substances, and pathogens
Cellular renewal time for a gastric surface mucous cell is approximately 3 days • The surface epithelial lining is invaginated by gastric pits or foveolae, that provide the gastric glands access to the gastric lumen, with a ratio of 1 pit to 4 or 5 gastric glands. • The gastric glands of different anatomic regions of the stomach are lined with different types of specialized epithelial cells
The parietal cell(oxyntic cell) : in the neck, or isthmus, or in the oxyntic gland • The resting(unstimulated)parietal cell has prominent cytoplasmic tubulovesicles and intracellular canaliculi containing short microvilli along its apical surface • H+,K+ATPase is expressed in the tubulovesicle membrane upon cell stimulation, this membrane, along with apical membranes, transforms into a dense network of apical intracellular canaliculi containing long microvilli
Acid secretion, a process requiring high energy, occurs at the apical canalicular surface. • Numerous mitochondria (30–40% of total cell volume) generate the energy required for secretion.
Gastroduodenal Mucosal Defense • The gastric epithelium is under assault by endogenous noxious factors(hydrochloric acid (HCl), pepsinogen/pepsin, and bile salts)and exogenous substances(medications, alcohol, bacteria) • A highly intricate biologic system is in place to provide defense from mucosal injury and to repair any injury that may occur
The mucosal defense system as a three level barrier, preepithelial, epithelial, subepithelial elements • The first line : mucus-bicarbonate phospholipid layer (physicochemical barrier) to multiple molecules(hydrogen ions) • Mucus is secreted by gastroduodenal surface epithelial cells
water (95%) and a mixture of phospholipids and glycoproteins(mucin) • functions as a nonstirred water layer impeding diffusion of ions and molecules such as pepsin • The mucous gel Bicarbonate secreted in a regulated manner by surface epithelial cells of the gastroduodenal mucosa forms a pH gradient ranging from 1 to 2 at the gastric luminal surface and reaching 6 to 7 along the epithelial cell surfac
Next line defense : Surface epithelial cells • Several factors :mucus production, epithelial cell ionic transporter(maintain intracellular pH) and bicarbonate production, and intracellular tight junctions • heat shock proteins generate that prevent protein denaturation and protect cells from certain factors such as increased temperature, cytotoxic agents, or oxidative stress
If the preepithelial barrier were breached, gastric epithelial cells bordering a site of injury can migrate to restore a damaged region (restitution) • Independent of cell division and requires blood flow and an alkaline pH
Several growth factors EGF , TGFα, FGF modulate the process of restitution • Epithelial cell regeneration is regulated by prostaglandins and growth factors such as EGF and TGF-α • In epithelial cell renewal ,new vessels formation (angiogenesis) within the injured microvascular bed ,FGF and vascular endothelial growth factor (VEGF)
An elaborate microvascular system within submucosal layer is the key component of the subepithelial defense/repair system • providing HCO3−, which neutralizes the acid generated by the parietal cell ,adequate supply of micronutrients and oxygen while removing toxic metabolic by-products
Prostaglandins : central role in gastric epithelial defense/repair • Regulate the release of mucosal bicarbonate and mucus, inhibit parietal cell secretion, and are important in maintaining mucosal blood flow and epithelial cell restitution
Prostaglandins are derived from esterified arachidonic acid, which is formed from phospholipids (cell membrane) by the action of phospholipase A2 • A key enzyme that controls the rate-limiting step in prostaglandin synthesis is cyclooxygenase (COX), which is present in two isoforms (COX-1,COX-2), each having distinct characteristics regarding structure, tissue distribution, and expression
COX-1 is expressed in stomach, platelets, kidneys, and endothelial cells , constitutive manner and important role in maintaining the integrity of renal function, platelet aggregation, and gastrointestinal (GI) mucosal integrity • COX-2 is inducible by inflammatory stimuli, expressed in macrophages, leukocytes, fibroblasts, and synovial cells • The beneficial effects of NSAIDs on tissue inflammation are due to inhibition of COX-2; the toxicity of these drugs (e.g., GI mucosal ulceration and renal dysfunction) is related to inhibition of the COX-1 isoform
The highly COX-2–selective NSAIDs have the potential beneficial effect of decreasing tissue inflammation while minimizing toxicity in the GI tract • Selective COX-2 inhibitors have had adverse effects on the cardiovascular system(MI) • FDA has removed (valdecoxib and rofecoxib)
Nitric oxide (NO) is important in the maintenance of gastric mucosal integrity • The key enzyme NO synthase is expressed in the mucosa and cytoprotection by stimulating gastric mucus, increasing mucosal blood flow, and maintaining epithelial cell barrier function • CNS and hormonal factors also play a role in regulating mucosal defense through multiple pathways
Physiology of Gastric Secretion • Hydrochloric acid and pepsinogen ,two principal gastric secretory , inducing mucosal injury • They have physiologic role in protein digestion; absorption of iron, calcium, magnesium, and vitamin B12; and killing ingested bacteria • Acid secretion should be viewed under basal and stimulated conditions • Basal acid production : circadian pattern, with highest levels occurring during the night and lowest levels during the morning hours • Cholinergic input (vagus) and histaminergic input (local gastric sources)principal contributors to basal acid secretion
Stimulated gastric acid : occurs in three phases • cephalic, gastric, and intestinal • Cephalic phase :Sight, smell, and taste of food … stimulates vagus nerve… gastric secretion • Gastric phase : once food enters the stomach • Directly stimulate G cell by nutrients (amino acids and amines)… release gastrin… activates parietal cell(via direct and indirect mechanisms)
Distention of stomach wall … gastrin release • The last phase : intestine food enters … luminal distention and nutrient assimilation
A series of pathways that inhibit gastric acid production are also set into motion during these phases • Somatostatin , GI hormone , from endocrine cells in gastric mucosa (D cells) in response to HCl , inhibit acid production by both direct (parietal cell) and indirect mechanisms (decreased histamine release from ECL cells and gastrin release from G cells)
Additional neural (central and peripheral) and humoral (amylin, atrial natriuretic peptide [ANP], cholecystokinin, ghrelin, interleukin 11 [IL-11], obestatin, secretin, and serotonin) factors play a role in counterbalancing acid secretion. • Under physiologic circumstances, these phases occur simultaneously • Ghrelin, the appetite-regulating hormone expressed in Gr cells in the stomach … increase gastric acid secretion …through stimulation of histamine release from ECL cells
parietal cell(acid-secreting) …located in oxyntic gland … adjacent to ECL cell, D cell…IF and IL-11…expresses receptors for several stimulants of acid secretion(histamine (H2), gastrin (cholecystokinin B/gastrin receptor), and acetylcholine (muscarinic,M3) • Binding of histamine to the H2 receptor .. activation of adenylate cyclase … increase in cyclic AMP
Activation of the gastrin and muscarinic receptors results in activation of the protein kinase C/phosphoinositide signaling pathway • Each of these signaling pathways in turn regulates a series of downstream kinase cascades that control the acid-secreting pump, H+,K+-ATPase
The enzyme H+,K+-ATPase is responsible for generating the large concentration of H+ • It is a membrane-bound protein that consists of two subunits, α and β • The active catalytic site is found within the α subunit; the function of the β subunit is unclear • This enzyme uses ATP to transfer H+ ions from parietal cell cytoplasm to the secretory canaliculi in exchange for K+
The H+,K+-ATPase is located within the secretory canaliculus and in nonsecretory cytoplasmic tubulovesicles • The tubulovesicles are impermeable to K+ • The distribution of pumps between the nonsecretory vesicles and the secretory canaliculus varies according to parietal cell activity • Proton pumps are recycled back to the inactive state in cytoplasmic vesicles once parietal cell activation ceases
The chief cell, in gastric fundus, synthesizes and secretes pepsinogen(inactive precursor) , proteolytic enzyme pepsin • The acid environment leads to cleavage of the inactive precursor to pepsin and provides the low pH (<2) required for pepsin activity • Pepsin activity is significantly diminished at a pH of 4 and irreversibly inactivated and denatured at a pH of ≥7 • Many of the secretagogues that stimulate acid secretion also stimulate pepsinogen release • The precise role of pepsin in the pathogenesis of PUD remains unknown