Download

1 / 18
180 likes | 249 Views
Learn about the characteristics, classification, epidemiology, transmission, pathogenesis, clinical manifestations, and complications of Rubella. Understand the impact on pregnant women, infants, and potential long-term effects.

E N D
Rubella Dr hab.n. med. Ewa Majda - Stanisławska Department of infectious Diseases and Hepatology Medical University of Lodz
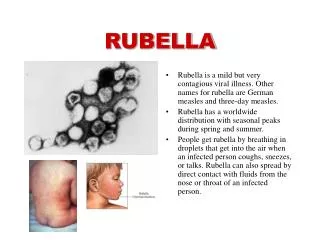
Rubella • characterized by rash, fever, and lymphadenopathy and resembles a mild case of measles (rubeola). • many infections with the agent are subclinical, • this virus has the potential to cause fetal infection, with resultant birth defects, • uncommonly, but especially in adults, may cause various forms of arthritis.
Classification • Rubella virus is classified in the Togaviridae family • placed in a separate genus, Rubivirus. • RNA virus, icosahedral capsid, and lipoprotein envelope.
Epidemiology • Epidemics of rubella of minor proportions occurred in the prevaccine era every 6 to 9 years, and large-scale epidemics occurred at intervals of up to 30 years. The most recent major epidemic in the United States occurred in 1964, during which some 12500000 persons were infected
Transmission • Rubella virus is spread in droplets that are shed from respiratory secretions of infected persons. • Patients are most contagious while the rash is erupting, • They may shed virus from the throat from 10 days before until 15 days after the onset of the rash. • Patients with subclinical cases of illness may also transmit the infection to others.
Transmission in case of congenital rubella • Infants with congenital rubella shed large quantities of virus from body secretions for many months and therefore may transmit the infection to those who care for them. • These babies continue to excrete rubella virus despite high titre of neutralizing antibody, a puzzling phenomenon that has yet to be explained • The possibility of immune tolerance due to fetal infection has been raised.
Pathogenesis • The incubation period for rubella ranges from 12 to 23 days (average, 18 days). • As in measles a primary and a secondary viremia are believed to accompany rubella. • Rubella virus has been detected in leukocytes of patients as early as 1 week before the onset of symptoms. • The rubella rash appears as immunity develops and the virus disappears from the blood, suggesting that the rash is immunologically mediated
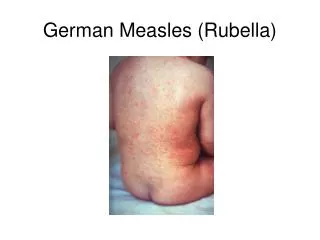
Clinical manifestations - rash • Begins on the face and moves down the body • It is maculopapular but not confluent, • May desquamate during convalescence, • May be absent in some cases. • An enanthem consisting of petechial lesions on the soft palate (Forscheimer's spots) has been described for rubella, • This enanthem is not diagnostic for rubella (unlike Koplik's spots in measles). • The rash may be accompanied by mild coryza and conjunctivitis. • Usually the rash lasts 3 to 5 days. • Fever, if present, rarely lasts beyond the first day of rash.
Differential diagnosis of rubella • measles, • toxoplasmosis, • scarlet fever, • roseola, • parvovirus B19 infection, • certain enterovirus infections • monocytic angina
Complications of postnatal Rubella- arthritis • Arthritis or arthralgia has been reported in as many as one third of women with rubella; • this complication is less common in children and in men. • The arthritis tends to involve the fingers, wrists, and knees, and it occurs either as the rash is appearing or soon afterward. • It can be rather slow to resolve, as long as 1 month. • Rarely does chronic arthritis develop.
Complications of postnatal Rubella- hemorrhagic manifestations • occur in approximately 1 of every 3000 cases of rubella. • occur more often in children than in adults • may be secondary to both thrombocytopenia and vascular damage, • they are more is probably immunologically mediated • thrombocytopenia may last from weeks to months and may cause serious problems if bleeding into vital areas (e.g., brain, kidney, eye) occurs
Congenital rubella • Can lead to fetal death, premature delivery, and an array of congenital defects • The rubella epidemic of 1964 left 30000 affected infants
Congenital rubella • The effects of rubella virus on the fetus are dependent on the time of infection; • During the first 2 months of gestation, the fetus has a 65% to 85% chance of being affected, with an outcome of multiple congenital defects, spontaneous abortion, or both. • Rubella during the third month of fetal life is associated with a 30% to 35% chance of developing a single defect, such as deafness or congenital heart disease. • Fetal infection during the fourth month carries a 10% risk of a single congenital defect. • Occasionally, fetal damage (deafness alone) is seen if rubella occurs up to the 20th week of gestation.
Congenital rubella • Diabetes mellitus in late childhood has also been observed 50 times more frequently in children who had congenital rubella than in normal children
Clinical manifestations - postnatal rubella • Many cases of postnatal rubella are subclinical • Children do not experience a prodromal phase, • Adults may have a prodrome of malaise, fever, and anorexia for several days • The major clinical manifestations of postnatal rubella are: • adenopathy, which may last several weeks (the posterior auricular, posterior cervical, and suboccipital chains. the posterior auricular, posterior cervical, and suboccipital chains) • rash. • on occasion, splenomegaly
Diagnosis of rubella • The diagnosis of congenital rubella infection has been made by isolation of virus from amniotic fluid • The laboratory diagnosis of postnatal rubella is most conveniently made serologically (ELISA) • For a serologic diagnosis of congenital rubella in the neonatal period, antibody to rubella virus should be measured in both infant and maternal sera
Treatment • no treatment for postnatal rubella • for patients with fever and arthritis or arthralgia, the treatment of symptoms is indicated. • immune globulin (IG) was advocated for the prevention or modification of rubella in susceptible pregnant women who were exposed to the infection, although it would not necessarily prevent viremia. • IG may be given to a susceptible pregnant woman who are exposed to rubella and for whom abortion is not an option, when they develop the disease. • rubella vaccine- immunization of susceptible women of childbearing age before they become pregnant.