Download
1 / 63
630 likes | 828 Views
Hypothyroidism Following Hemithyroidectomy. By : Dr. Shirley Y. Su, MBBS. Dr. Simon Grodski, MBBS, FRACS. Dr. Jonathan W. Serpell, MBBS, FRACS. Presented By : Under supervision of : Dr. Naef Al haddy Dr. Abdulhakim Tamimi. Permission.

E N D
Hypothyroidism Following Hemithyroidectomy By : Dr. Shirley Y. Su, MBBS. Dr. Simon Grodski, MBBS, FRACS. Dr. Jonathan W. Serpell, MBBS, FRACS. Presented By : Under supervision of : Dr. Naef Al haddy Dr. Abdulhakim Tamimi
Permission Dear Dr. Naef Al Haddy, • You are welcome to present my paper at your journal club. • Thank you for your interest. • Regards, • Shirley Su • On Tue, Jan 5, 2010 at 2:15 AM, scientific committee <sc_4all@yahoo.com> wrote: • Dear Dr . shirley • We are in Yemen – Aden , and we have a journal club in 11/ 01/ 2010 , and we like to present your
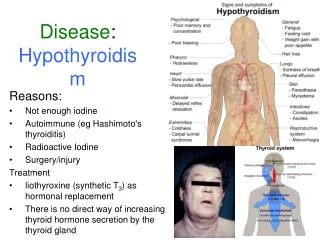
Background • The incidence & risk factors for hypothyroidism in patients undergoing partial thyroid surgery remains unclear. With reported rates up to 60% in the literature • Hypothyroidism is defined biochemically by elevated TSH ( normal 0.5 – 4.0 mIU/L )
Background • Hypothyroidism is an under appreciated sequel of hemithyroidectomy. • The early recognition of this postoperative complication may prevent symptoms of hypothyroidism and recurrent thyroid disease.
Objective • To investigate the incidence. • Time to onset. • Risk factors for the development of hypothyroidism after hemithyroidectomy
Methods • We conducted a retrospective review of all patients undergoing hemithyroidectomy from August 1992 to June 2006 by a single surgeon.
Methods Patients were analyzed for • age • sex • family history of thyroid disease • thyroid antibody levels • pre- and postoperative thyroid stimulating hormone (TSH)
Methods • histologic diagnosis • weight of resected tissue • histologic evidence of thyroiditis • and lag time to diagnosis of hypothyroidism.
Results • operated cases 490 cases 196 excluded , 294 available for analysis • Hypothyroidism was diagnosed in ( 32 ) 10.9% of 294 patients and 262 euthyroid .
Results • The main TSH is significantly different b/w euthyroid group ( 2.1 ± 1.1 mIU/L ) hypothyroid group ( 9.3 ± 4.9 mIU/L ) • The mean time to diagnosis was (8.2 months)
Results • Patients with postoperative hypothyroidism had a higher incidence of: • high-normal preoperative TSH level (TSH: 2.5-4.0 mIU/L),(18.8% vs. 3.8%;) P < 0.01
Results • -thyroiditis on histology (46.8% vs. 11.8%;) P < 0.01 and • -elevated thyroid antibodies levels (47.8% vs. 11.5%;) P < 0.01.
Results • Age, gender, family history of thyroid disease, thyroid pathology, and weight of resected tissue were not significant risk factors for hypothyroidism
Discussion • Hypothyroidism after hemethyroidectomy is a poorly anticipated complication, dispite a reported incidence of b/w 6.5% & 45% and up to 65% in patient with head and neck ca .
Discussion • Risk factors in previous studies have variously attributed to the presence of (anti-TPO antibody , thyroiditis , multinodular goiter , preoperative thyrotoxicosis & thyroid remnant < 6 g.
Discussion • In our study the most important risk factors are : thyroiditis, anti – TPO antibody & preoperative (TSH level : 2.5-4.0 mIU/L). • In previous studies hypothyroidism more prevalent among elderly patients, but in this study no significant difference b/w eu. & hypo. (49.5 vs 54.5 y).
Discussion • Regarding the pathology of resected tissue the only difference is in cases of multinodular goiter ( 26.3% vs 34.4% ) but not so significant .
Preoperative TSH level • Patient with elevated TSH level were excluded • In Patient with Preoperative normal TSH level , the proportion of postoperative hypothyroidism patients is similar to Euthyroid patients (84.4% vs 83.9%).
Preoperative TSH level • when patients stratified into 2 groups ( TSH 0.5 – 2.4 & TSH 2.5 – 4.0 mIU/L ) a higher proportion of patient who develop hypothyroidism had TSH in the higher end of normal rang .
Preoperative thyroid antibody • Preoperative thyroid antibody was done in 58.2% of patients ( 148 in euthyroid patient & 23 in the hypothyroid group ) • The most common was ( antithyroid peroxidase ) anti – TPO antibody .
Preoperative thyroid antibody • elevated thyroid antibody In 47.8% of patient developed postoperative hypothyroidism , • 11.5% remained euthyroid.
Thyroiditis • 46 cases had thyroiditis (3 primary Hashimoto,s & 43 secondary with primary pathology ) • A significantly higher proportion of patient in the postoperative hypothyroid group had Thyroiditis as compared with those in the euthyroid group ( 46.8% vs 11.8% )
Predictors of Hypothyroidism Hypothyroidism Hyperthyroidism
Predictors of Hypothyroidism Postoperative hypothyroidism was observed to develop in : • 39.3% of patient with thyroid antibody , • 32.6% wth thyroiditis ,and • 37.5% with TSH b/w 2.5 – 4.0 mIU/L.
Predictors of Hypothyroidism • patients with anti – TPO antibody had an even higher incidence 46.7%
Predictors of Hypothyroidism • the presence of thyroiditis on histopathology was the most sensitive indicator of postoperative hypothyroidism 47% .
Predictors of Hypothyroidism • the combined presence of Anti- TPO antibody , thyroiditis , TSH b/w 2.5 – 4.0 mIU/L had a much higher positive predictive value 80% than any single factor .
Predictors of Hypothyroidism • Patients with -ve antibody only 8.4% , • without thyroiditis 6.85% or • preoperative TSH < 2.5 mIU/L 9.1% - 10.6% .
Hyperthyroidism Hypothyroidism Hypothyroid patients
Hypothyroidism: S&S Cardiovascular: Slow Heartbeat Elevated Cholesterol Aging: Dry, Scaly Skin Sparse or Coarse Hair Ear, Nose & Throat: Hoarse Voice Gynecological: Irregular menstruation Infertility
Hypothyroidism: S&S Gastrointestinal: Constipation Weight Gain Psychiatric: Impaired Concentration Depression Lethargy, Fatigue Muscular: Muscle Weakness Stiffness Blood: Anemia
Hypothyroid patients • Time at diagnosis 68% by 6 months , 90% by 15 months • Maine time to diagnosis was 8.2 months , • The maine TSH at diagnosis was 9.3 ± 4.9 mIU/L .
Hypothyroid patients • Majority of patients had subclinical hypothyroidism 78.1% • Four patients 12.5% had transient postoperative hypothyroidism .
Hypothyroid patients • Only patients with overt hypothyroidism ( low free T4 and elevated TSH ), together with patients with signs or symptoms of hypothyroidism (with elevated TSH ) were commenced on thyroxine treatment .