Download
1 / 1
10 likes | 105 Views
CORODONT. AC number of 16S rRNA sequence. Characteristic. Cases (n=263). Controls (n=526). Length. Species. Sequence of probe (5‘ to 3‘) . Male (%) †. 87. 87. Mean Age (years), (SD) †. 61.0 (7.1). 61.0 (7.1). M75035. A. actinomycetemcomitans. cac tta aag gtc cgc cta cgt gcc. 24.

E N D
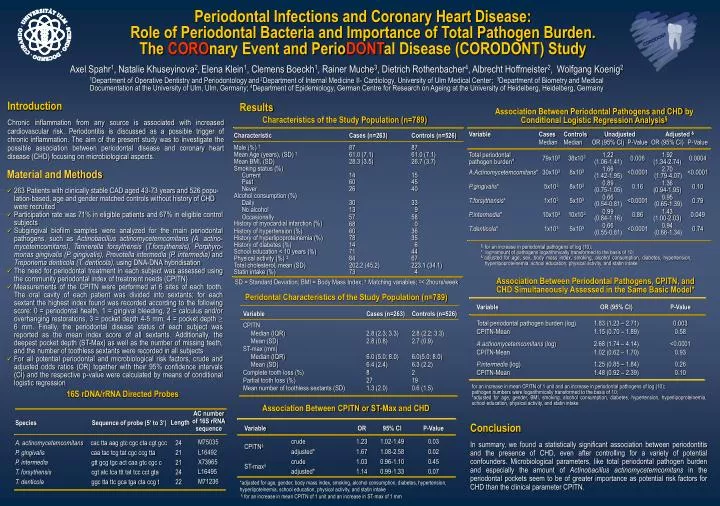
CORODONT AC numberof 16S rRNAsequence Characteristic Cases (n=263) Controls (n=526) Length Species Sequence of probe (5‘ to 3‘) Male (%) † 87 87 Mean Age (years), (SD) † 61.0 (7.1) 61.0 (7.1) M75035 A. actinomycetemcomitans cac tta aag gtc cgc cta cgt gcc 24 Mean BMI, (SD) 28.3 (3.5) 26.7 (3.7) L16492 P. gingivalis caa tac tcg tat cgc ccg tta 21 Smoking status (%) X73965 P. intermedia gtt gcg tgc act caa gtc cgc c 21 Current 14 15 Past 60 45 L16495 T. forsythensis cgt atc tca ttt tat tcc cct gta 24 Never 26 40 M71236 T. denticola ggc tta ttc gca tga cta ccg t 22 Alcohol consumption (%) Daily 30 33 No alcohol 13 9 Occasionally 57 58 History of myocardial infarction (%) 68 0 History of hypertension (%) 60 36 History of hyperlipoproteinemia (%) 78 35 Association Between Periodontal Pathogens, CPITN, and CHD Simultaneously Assessed in the Same Basic Model* History of diabetes (%) 14 6 School education < 10 years (%) 71 44 Physical activity (%) ‡ 84 67 Total cholesterol, mean (SD) 202.2 (45.2) 223.1 (34.1) Statin intake (%) 73 4 SD = Standard Deviation; BMI = Body Mass Index; † Matching variables; ‡< 2hours/week Periodontal Infections and Coronary Heart Disease: Role of Periodontal Bacteria and Importance of Total Pathogen Burden. The COROnary Event and PerioDONTal Disease (CORODONT) Study Peridontal Characteristics of the Study Population (n=789) Axel Spahr1, Natalie Khuseyinova2,Elena Klein1, Clemens Boeckh1, Rainer Muche3, Dietrich Rothenbacher4, Albrecht Hoffmeister2, Wolfgang Koenig2 1Department of Operative Dentistry and Periodontologyand 2Department of Internal Medicine II- Cardiology, University of Ulm Medical Center; 3Department of Biometry and Medical Documentation at the University of Ulm, Ulm, Germany; 4Department of Epidemiology, German Centre for Research on Ageing at the University of Heidelberg, Heidelberg, Germany Introduction Chronic inflammation from any source is associated with increased cardiovascular risk. Periodontitis is discussed as a possible trigger of chronic inflammation. The aim of the present study was to investigate the possible association between periodontal disease and coronary heart disease (CHD) focusing on microbiological aspects. Results Association Between Periodontal Pathogens and CHD by Conditional Logistic Regression Analysis§ Characteristics of the Study Population (n=789) • Material and Methods • 263 Patients with clinically stable CAD aged 43-73 years and 526 popu-lation-based, age and gender matched controls without history of CHD were recruited • Participation rate was 71% in eligible patients and 67% in eligible control subjects • Subgingival biofilm samples were analyzed for the main periodontal pathogens, such as Actinobacillus actinomycetemcomitans (A. actino-mycetemcomitans), Tannerella forsythensis (T.forsythensis), Porphyro-monas gingivalis (P. gingivalis), Prevotella intermedia (P. intermedia) and Treponema denticola (T. denticola), using DNA-DNA hybridisation • The need for periodontal treatment in each subject was assessed using the community periodontal index of treatment needs (CPITN) • Measurements of the CPITN were performed at 6 sites of each tooth. The oral cavity of each patient was divided into sextants; for each sextant the highest index found was recorded according to the following score: 0 = periodontal health, 1 = gingival bleeding, 2 = calculus and/or overhanging restorations, 3 = pocket depth 4-5 mm, 4 = pocket depth 6 mm. Finally, the periodontal disease status of each subject was reported as the mean index score of all sextants. Additionally, the deepest pocket depth (ST-Max) as well as the number of missing teeth, and the number of toothless sextants were recorded in all subjects • For all potential periodontal and microbiological risk factors, crude and adjusted odds ratios (OR) together with their 95% confidence intervals (CI) and the respective p-value were calculated by means of conditional logistic regression § for an increase in periodontal pathogens of log (10); * log=amount of pathogens logarithmically transformed to the basis of 10; & adjusted for age, sex, body mass index, smoking, alcohol consumption, diabetes, hypertension, hyperlipoproteinemia, school education, physical activity, and statin intake for an increase in mean CPITN of 1 unit and an increase in periodontal pathogens of log (10); pathogen numbers were logarithmically transformed to the basis of 10; *adjusted for age, gender, BMI, smoking, alcohol consumption, diabetes, hypertension, hyperlipoproteinemia, school education, physical activity, and statin intake 16S rDNA/rRNA Directed Probes Association Between CPITN or ST-Max and CHD Conclusion In summary, we found a statistically significant association between periodontitis and the presence of CHD, even after controlling for a variety of potential confounders. Microbiological parameters, like total periodontal pathogen burden and especially the amount of Actinobacillusactinomycetemcomitans in the periodontal pockets seem to be of greater importance as potential risk factors for CHD than the clinical parameter CPITN. *adjusted for age, gender, body mass index, smoking, alcohol consumption, diabetes, hypertension, hyperlipoteinemia, school education, physical activity, and statin intake§ for an increase in mean CPITN of 1 unit and an increase in ST-max of 1 mm