Download
1 / 30
300 likes | 438 Views
Update on Anti-platelets. Gabriel A. Vidal, MD Vascular Neurology Ochsner Medical Center October 14 th , 2009. Primary Stroke Prevention. Primary Vascular Disease Prevention Primary Prevention Trials Meta-Analysis Lancet 2009; 373:1849-60. Meta-analysis for serious vascular events

E N D
Update on Anti-platelets Gabriel A. Vidal, MD Vascular Neurology Ochsner Medical Center October 14th, 2009
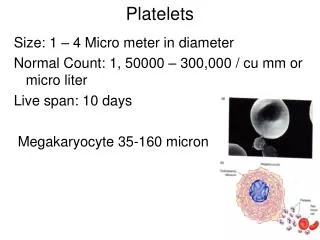
Primary Vascular Disease PreventionPrimary Prevention Trials Meta-AnalysisLancet 2009; 373:1849-60 • Meta-analysis for serious vascular events • MI, CI, VD • Major bleeding • 6 primary prevention trials = 95,000 individuals • Aspirin trials: • 12% reduction in vascular events • Statistically significant • MI reduced 1/5 • No effect on stroke, hemorrhagic stroke, vascular death • Effect similar for men and women
Primary Vascular Disease PreventionPrimary Prevention Trials Meta-AnalysisLancet 2009; 373:1849-60
Primary Vascular Disease PreventionPrimary Prevention Trials Meta-AnalysisLancet 2009; 373:1849-60
Clinical Trials • CAST - Chinese Acute Stroke Trial (1997) • Randomized, placebo-controlled trial of 21,106 patients • 10,554 patients were randomized to receive aspirin (160 mg/day) and 10,552 received placebo • Significant (14%) reduction in mortality and fewer recurrent ischemic strokes in patients receiving aspirin during treatment period • At discharge, 11.4 fewer patients per 1000 were dead or dependent in the group receiving aspirin • IST - International Stroke Trial (1997) • Randomized, open trial involving 19435 patients • Half of the participating patients received unfractionated heparin and half were told to avoid heparin • In a factorial design, half received aspirin 300 mg daily and half were told to avoid aspirin • No statistically significant difference in death at 14 days, or death or dependence at 6 months between patients receiving heparin vs. no heparin • Statistically significant difference in the number of deaths and recurrent strokes between patients receiving aspirin vs. no aspirin • Taken together, CAST and IST show reliably that aspirin started early in hospital produces a small but definite net benefit • About 9 fewer deaths or non-fatal strokes per 1000 in the first few weeks • About 13 fewer dead or dependent per 1000 after some weeks or months of follow-up
Clinical Trials • ESPS2 – European Stroke Prevention Study 2 (1996) • Patients were randomized to participate in 1 of 4 groups • 24-month stroke rate (Statistically significant) • 12.9% in the aspirin-alone group (18% risk reduction) • 12.2% in the dipyridamole-alone group (16% risk reduction) • 9.9% in the combination group (37% risk reduction vs placebo; 23% vs. ASA) • 15.8% in the placebo group • No significant difference among the groups for the endpoint of death • ESPIRIT - European / Australasian Stroke Prevention in Reversible Ischemia Trial (2006) • Anticoagulants versus aspirin comparison of ESPRIT • Prematurely ended because ESPRIT reported that the combination of aspirin and dipyridamole was more effective than aspirin alone • Primary outcome events arose in 13% patients on combination treatment vs. 16% on aspirin alone • Hazard ratio for the primary outcome event comparing anticoagulants with the combination treatment of aspirin and dipyridamole was 1.31, for ischemic events was 0.73 and for major bleeding complications 2.56 • Patients on the combination of aspirin and dipyridamole discontinued trial medication more often than those on aspirin alone, mainly because of headache
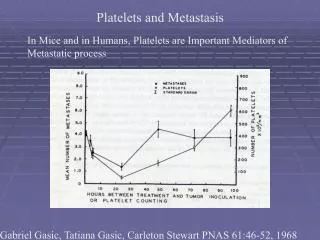
ESPIRITPrimary outcome: nonfatal CI, MI, vascular death, major bleedingLancet, 2006
Aspirin + DipyridamoleMeta-analysisVerro, Stroke, 2008 Non-fatal stroke endpoint Composite endpoint of nonfatal CI, MI, or vascular death
Aspirin + DipyridamoleMeta-analysis: Non-fatal stroke endpointImmediate Release VS Extended Release (Verro, Stroke, 2008) Immediate releasetrials Extended release trials
Clinical Trials • WARSS – Warfarin vs Aspirin Recurrent Stroke Study (2001) • Randomized to receive either aspirin (325 mg/day) or warfarin (INR 1.4-2.8) for at least two years • Primary end point of death or recurrent ischemic stroke was reached by 17.8% of patients assigned to warfarin and 16% of those assigned to aspirin • Rates of major hemorrhage were low (2.22 per 100 patient-years in the warfarin group and 1.49 in the aspirin group) • There were no statistical differences in primary or secondary endpoints or in major hemorrhage • WASID – Warfarin vs Aspirin Symptomatic Intracranial Disease (2005) • Randomized to receive either aspirin 1300 mg/day or warfarin, titrated to an INR of 2 - 3 • There was 4.3% rate of death in the aspirin group and a 9.7% rate in the warfarin group • There was a 3.2% rate of major hemorrhage in the aspirin group and a 8.3% rate in the warfarin group • The primary end point occurred in 22.1 percent of the patients in the aspirin group and 21.8 percent of those in the warfarin group
Clinical Trials • CAPRIE – Clopidogrel vs Aspirin in Patients at Risk for Ischaemic Events (1996) • Randomized double dummy Clopidogrel 75 mg vs Aspirin 325 mg • Patients treated with clopidogrel had a 5.32% annual risk of ischemic stroke, myocardial infarction or vascular death vs 5.83% in patients treated with aspirin • Statistically significant relative-risk reduction of 8.7% in favor of clopidogrel • MATCH – Management of ATherothrombosis with Clopidogrel in High-risk patients with recent TIA or ischemic stroke (2004) • Randomized to Clopidogrel + ASA or Clopidogrel + placebo • Compared to clopidogrel, combination with ASA had no significant effect on recurrent ischemic events • 15.7% of patients taking combination had a further ischemic event vs 16.73% of patients taking clopidogrel + placebo • Patients taking clopidogrel + ASA also had significantly more life-threatening hemorrhage vs patients taking clopidogrel + placebo • CHARISMA – Clopidogrelfor High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (2006) • Randomized to receive either clopidogrel or placebo, in combination with aspirin • Clopidogrel plus aspirin was not significantly more effective than aspirin alone in reducing the rate of myocardial infarction, stroke, or death from cardiovascular causes
Clinical Trials • PRoFESS – Prevention Regimen For Effectively avoiding Second Strokes (2008) • 18,500 patients will be randomized to receive active antiplatelet medication, either clopidogrel or extended-release dipyridamole and aspirin • Primary Outcome: Time to first recurrent stroke • Recurrent strokes occurred in 9% patients randomly assigned to ASA with ER-DP and 9% patients randomly assigned to clopidogrel • mRS scores were not statistically different in patients with recurrent stroke who were treated with ASA and ER-DP versus clopidogrel • There was no significant difference in the proportion of patients with recurrent stroke with a good outcome, as measured with the Barthel index, across all treatment groups • There is no evidence that either of the two treatments was superior to the other in the prevention of recurrent stroke