Download
1 / 1
10 likes | 139 Views
Health Resume for Our Pregnant Moms. Today’s Date ___________________ Name ________________________________________ Birth date _______________ Age _____ Gender M F Address ______________________________________ City ____________________ State ____ Zip _________

E N D
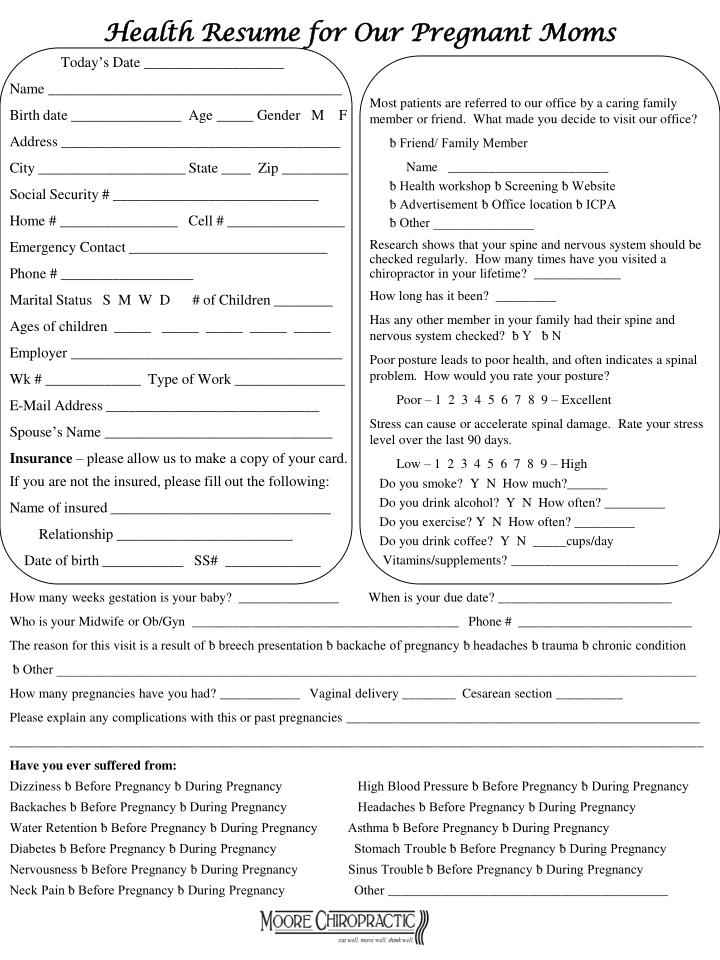
Health Resume for Our Pregnant Moms Today’s Date ___________________ Name ________________________________________ Birth date _______________ Age _____ Gender M F Address ______________________________________ City ____________________ State ____ Zip _________ Social Security # ____________________________ Home # ________________ Cell # ________________ Emergency Contact ___________________________ Phone # __________________ Marital Status S M W D # of Children ________ Ages of children _____ _____ _____ _____ _____ Employer _____________________________________ Wk # _____________ Type of Work _______________ E-Mail Address _____________________________ Spouse’s Name _______________________________ Insurance – please allow us to make a copy of your card. If you are not the insured, please fill out the following: Name of insured ______________________________ Relationship ________________________ Date of birth ___________ SS# _____________ Most patients are referred to our office by a caring family member or friend. What made you decide to visit our office? ƀ Friend/ Family Member Name ________________________ ƀ Health workshop ƀ Screening ƀ Website ƀ Advertisement ƀ Office location ƀ ICPA ƀ Other _______________ Research shows that your spine and nervous system should be checked regularly. How many times have you visited a chiropractor in your lifetime? _____________ How long has it been? _________ Has any other member in your family had their spine and nervous system checked? ƀ Y ƀ N Poor posture leads to poor health, and often indicates a spinal problem. How would you rate your posture? Poor – 1 2 3 4 5 6 7 8 9 – Excellent Stress can cause or accelerate spinal damage. Rate your stress level over the last 90 days. Low – 1 2 3 4 5 6 7 8 9 – High Do you smoke? Y N How much?______ Do you drink alcohol? Y N How often? _________ Do you exercise? Y N How often? _________ Do you drink coffee? Y N _____cups/day Vitamins/supplements? _________________________ How many weeks gestation is your baby? _______________ When is your due date? __________________________ Who is your Midwife or Ob/Gyn ________________________________________ Phone # __________________________ The reason for this visit is a result of ƀ breech presentation ƀ backache of pregnancy ƀ headaches ƀ trauma ƀ chronic condition ƀ Other ________________________________________________________________________________________________ How many pregnancies have you had? ____________ Vaginal delivery ________ Cesarean section __________ Please explain any complications with this or past pregnancies _____________________________________________________ ________________________________________________________________________________________________________ Have you ever suffered from: Dizziness ƀ Before Pregnancy ƀ During Pregnancy High Blood Pressure ƀ Before Pregnancy ƀ During Pregnancy Backaches ƀ Before Pregnancy ƀ During Pregnancy Headaches ƀ Before Pregnancy ƀ During Pregnancy Water Retention ƀ Before Pregnancy ƀ During Pregnancy Asthma ƀ Before Pregnancy ƀ During Pregnancy Diabetes ƀ Before Pregnancy ƀ During Pregnancy Stomach Trouble ƀ Before Pregnancy ƀ During Pregnancy Nervousness ƀ Before Pregnancy ƀ During Pregnancy Sinus Trouble ƀ Before Pregnancy ƀ During Pregnancy Neck Pain ƀ Before Pregnancy ƀ During Pregnancy Other __________________________________________