Download
1 / 77
1.07k likes | 2.12k Views
Blood-Hematopoiesis-Lymphatics 2013. Multiple Myeloma & Related Plasma Cell Dyscrasias. William Kern, MD Director, Clinical Hematopathology william-kern@ouhsc.edu. Downloading any of the photographs, graphs or diagrams from this presentation is prohibited. Monoclonal Gammopathies.

E N D
Blood-Hematopoiesis-Lymphatics 2013 Multiple Myeloma & Related Plasma Cell Dyscrasias William Kern, MD Director, Clinical Hematopathology william-kern@ouhsc.edu
Downloading any of the photographs, graphs or diagrams from this presentation is prohibited.
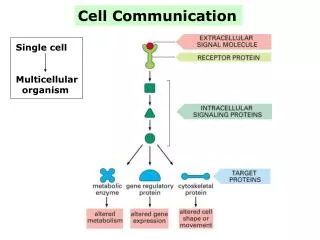
Monoclonal Gammopathies • Disorders associated with production of a monoclonal immunoglobulin protein: • Multiple myeloma & variants • Monoclonal gammopathy of undetermined significance (MGUS) • Waldenström macroglobulinemia • Primary (AL) amyloidosis • Non-Hodgkin lymphomas (occasional cases)
Monoclonal Gammopathies WM/CLL= Waldenström’s Macroglobulinemia/Chronic Lymphocytic Leukemia SOM/EMP = Solitary osseous myeloma/extramedullary plasmacytoma
Multiple Myeloma: Triad • Accumulation of plasma cells in bone marrow • Bone lesions • Monoclonal immunoglobulin protein in serum and/or urine
Multiple Myeloma: Epidemiology • Second most common malignancy of lymphoid cells overall • Most common lymphoid malignancy in African-Americans: • Twice as common in African-Americans as Caucasians • Predominantly occurs in older populations: • Median age ~70 at diagnosis
Multiple Myeloma: Etiology • Possible occupational exposures: • Increased in farmers, petroleum workers, wood & leather industries • Ionizing radiation: • Radiologists, nuclear plant workers, survivors of nuclear weapon explosions • No obvious predisposing factor in majority of cases
Multiple Myeloma • Heterogeneous • At least two biologic pathways • Variable clinical course: • May be indolent, with few symptoms & long survival • May be very aggressive, with severe symptoms and survival only a few years • Divided into symptomatic & asymptomatic variants
Symptomatic vs. Asymptomatic Myeloma • Symptomatic: • Presence of end-organ damage • Asymptomatic: • Significant level of monoclonal plasma cells in marrow • Significant level of monoclonal protein in serum or urine • No symptoms or end-organ damage
Multiple Myeloma: Diagnosis • Monoclonal protein in serum and/or urine: • Measure & determine type • Increased plasma cells in marrow • Presence of end-organ or tissue damage due to plasma cell proliferation or monoclonal immunoglobulin
Symptomatic Multiple Myeloma: Criteria • Presence of monoclonal plasma cell population in marrow • Monoclonal protein in serum and/or urine • Myeloma-related organ dysfunction (≥1): • Calcium elevation in blood • Renal insufficiency • Anemia • Lytic bone lesions or osteoporosis
Multiple Myeloma End-Organ Damage:CRAB C: hyperCalcemia R:Renal abnormalities A:Anemia B:Bone lesions
Multiple Myeloma:Common Laboratory Findings • Anemia: Common • Leukopenia, thrombocytopenia less common at diagnosis • Hypercalcemia • Renal insufficiency • Elevated total serum protein with normal or decreased serum albumin
Blood Smear: Rouleaux Downloaded from Jaffe ES et al, Hematopathology
Multiple Myeloma Bone marrow aspirate
Multiple Myeloma: Bone Lesions • Two types of bone lesions • “Punched out” osteolytic lesions: • Vertebrae, skull, ribs, pelvis, others • Present in ~60% of cases • Diffuse osteopenia: • May be missed on routine skeletal survey • CT or MRI may be more sensitive
Multiple Myeloma: Bone Lesions • Myeloma cells produce factors which stimulate osteoclasts to resorb bone: • Generically called “Osteoclast Activating Factor” (OAF) • Liberation of calcium from bone causes hypercalcemia Biphosphonates (Pamidronate) prevent bone breakdown
Multiple myeloma should be an important diagnostic consideration in any elderly patient with back pain plus anemia, renal insufficiency or elevated serum protein!!
Monoclonal Proteins • Monoclonal immunoglobulin: • “M-component,” “M-protein,” “M-spike” • Present in almost all cases: • Rare non-secretors (≤1%) • Intact immunoglobin ± light chain: • IgG ~50%; IgA ~25% • IgM, IgD & IgE all rare • Light chain only: ~10-25%
Detection of Monoclonal Proteins • Serum protein electrophoresis (SPEP): • Screening test • Separates based on charge & size • Also looks at other serum proteins • Immunofixation: • Identifies specific type • Free light chain assay
Serum Protein Electrophoresis Origin M i g r a t I o n Immunofixation
Serum Protein Electrophoresis: Densitometry Albumin M-Protein Migration
Light Chain-Only Myeloma • Light chain-only myeloma may be missed by routine SPEP: • Light chains are cleared by kidneys (“Bence Jones” protein) • Do not accumulate in plasma (serum) • A negative serum protein electrophoresis does not exclude myeloma!
Multiple Myeloma: Cytogenetics • Cytogenetics prognostically important in myeloma • Abnormalities often not detected by standard cytogenetics (G-banding) • Abnormalities are heterogeneous: • Aneuploidy of numerous chromosomes • Reciprocal translocations, usually involving 14q32 (IgH gene) This might come up on the USMLE….
Multiple Myeloma: Cytogenetics • Two major pathways: Aneuploidy and reciprocal translocations • Aneuploidy divided into hyperdiploid, pseudo-diploid, hypodiploid and near-tetraploid • Hyperdiploid is relatively favorable; the others (non-hyperdiploid) are relatively unfavorable
Multiple Myeloma: Cytogenetics • t(11;14) is most common translocation: • Results in dysregulation of cyclin D1 gene • Same translocation found in mantle cell lymphoma • Relatively favorable in multiple myeloma • t(4;14) is another common translocation: • Very unfavorable
Multiple Myeloma: Cytogenetics For reference – not memorization
Multiple Myeloma: Complications • Bone pain & fractures • Infection • Renal failure • Hypercalcemia
Multiple Myeloma: Infections • Most common cause of death • Predisposing factors: • Suppression of normal immunoglobulins • Immobility & general debilitation • Neutropenia: Due to marrow replacement and/or chemotherapy • Pneumonitis & pyelonephritis common • Strep. pneumoniae & Staph. aureus common
Multiple Myeloma: Renal Effects • Proteinuria common • Light chains (Bence Jones protein) + intact immunoglobulins • Nonspecific proteinuria also occurs • Note: Light chains not detected by routine urine dipstick: • Dipstick primarily detects albumin
Multiple Myeloma: Renal Effects • Renal insufficiency = second most common cause of death • Causes of renal damage: • Myeloma cast nephropathy • Light chains toxic to tubular cells • Hypercalcemia: Causes dehydration and renal stones • Hyperuricemia: Renal stones • Amyloidosis • Pyelonephritis
Multiple Myeloma: Renal Effects • Patients with multiple myeloma very sensitive to radiographic contrast agents or other nephrotoxic agents: • May induce renal shutdown • Be careful using radiographic contrast in elderly patients!
Multiple Myeloma: Treatment • No conventional therapy for myeloma is curative • Patients may respond to therapy for months or years • Eventually resistance develops • Survival thereafter is poor
Multiple Myeloma: Treatment • Old standard therapy: Phenylalanine mustard (Melphalan) + Prednisone (MP): • ~60-70% of patients respond • Thalidomide ± dexamethasone • Dexamethasone alone • Proteosome inhibitors (Velcade) Continued….
Multiple Myeloma: Newer Agents • Immunomodulatory drugs (IMiDs) • Lenalidomide (Revlimid) • Combination chemotherapy (VAD, others) • Bisphosphonates (Pamidronate): • Reduce fractures & bone pain
Multiple Myeloma: Stem Cell Transplant • Autologous: Widely used • Appears to prolong survival over conventional therapy • Generally well tolerated • Can be performed in older patients • Allogeneic: Potential for cure (?) • Many patients not eligible due to age • Significant morbidity & mortality rates • Currently considered experimental
Extramedullary Plasmacytoma • Plasma cell tumor outside of bone • Usually solitary • Upper respiratory tract = most common site • Usually no monoclonal protein in serum • Local therapy may be curative • Must exclude disseminated disease
Monoclonal Gammopathy of Undetermined Significance (MGUS) • Most common form of monoclonal gammopathy • Common in elderly populations • No clinical significance by itself Note: “MGUS” preferred over older term “Benign Monoclonal Gammopathy” (BMG)
MGUS: Definition • Monoclonal protein in absence of signs or symptoms of multiple myeloma: • No lytic bone lesions • <10% plasma cells in marrow • Low level of M-protein: • <3 g/dL in serum • Minimal M-protein in urine
MGUS: Transformation to Multiple Myeloma • ~25% transform to overt myeloma: • Median time ~8 years after diagnosis • May take ≥20 years • Transformation may be gradual or abrupt • Difficult to predict which patients will transform to overt myeloma: • Patients with higher M-protein levels at higher risk
MGUS: Treatment • No treatment for MGUS as such • Monitor serum and urine proteins, CBC, chemistry panel periodically • Treat for myeloma when & if overt myeloma develops
Waldenström Macroglobulinema (WM) • Monoclonal IgM protein in patient with lymphoplasmacytic lymphoma • Lymphoplasmacytic lymphoma = proliferation of cells intermediate between lymphocytes & plasma cells • IgM protein = “macroglobulin” • Clinical behavior resembles lymphoma more than typical myeloma
Waldenström’s Macroglobulinema Bone marrow aspirate; 100x oil immersion
Waldenström Macroglobulinema:Hyperviscosity Syndrome • Due to high levels of IgM protein • Symptoms: Fatigue, dizziness, blurred vision, shortness of breath • Exam: Dilated, “sausage-shaped” retinal veins Note: Hyperviscosity syndrome may occur in myeloma; IgA > IgG
Waldenström Macroglobulinema:Treatment • Plasmapheresis for hyperviscosity: • Rapidly reduces IgM level and serum viscosity • Chemotherapy needed prevent reaccumulation: • Chemotherapy as for CLL or low-grade non-Hodgkin lymphoma
Amyloidosis • Deposition of protein with beta-pleated sheet configuration in tissues • Variety of proteins may cause amyloidosis: • Immunoglobulin light chains or fragments • Serum amyloid-associated protein (SAA) • Prealbumin • Variety of hormones • Others