Download
1 / 1

E N D
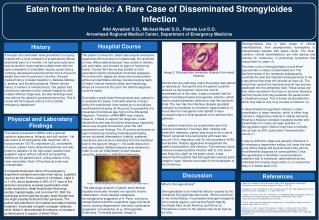
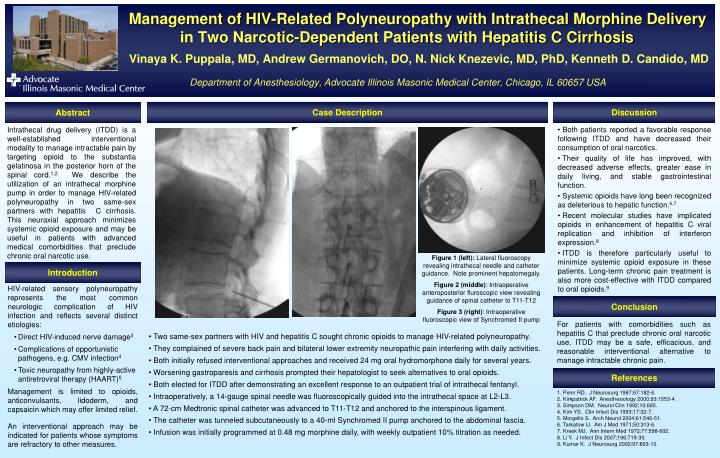
Management of HIV-Related Polyneuropathy with Intrathecal Morphine Delivery in Two Narcotic-Dependent Patients with Hepatitis C CirrhosisVinaya K. Puppala, MD, Andrew Germanovich, DO, N. Nick Knezevic, MD, PhD, Kenneth D. Candido, MDDepartment of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Case Description Discussion Abstract • Both patients reported a favorable response following ITDD and have decreased their consumption of oral narcotics. • Their quality of life has improved, with decreased adverse effects, greater ease in daily living, and stable gastrointestinal function. • Systemic opioids have long been recognized as deleterious to hepatic function.6,7 • Recent molecular studies have implicated opioids in enhancement of hepatitis C viral replication and inhibition of interferon expression.8 • ITDD is therefore particularly useful to minimize systemic opioid exposure in these patients. Long-term chronic pain treatment is also more cost-effective with ITDD compared to oral opioids.9 Intrathecal drug delivery (ITDD) is a well-established interventional modality to manage intractable pain by targeting opioid to the substantia gelatinosa in the posterior horn of the spinal cord.1,2We describe the utilization of an intrathecal morphine pump in order to manage HIV-related polyneuropathy in two same-sex partners with hepatitis C cirrhosis. This neuraxial approach minimizes systemic opioid exposure and may be useful in patients with advanced medical comorbidities that preclude chronic oral narcotic use. Figure 1 (left): Lateral fluoroscopy revealing intrathecal needle and catheter guidance. Note prominent hepatomegaly. Figure 2 (middle): Intraoperative anteroposterior fluroscopic view revealing guidance of spinal catheter to T11-T12 Figure 3 (right): Intraoperative fluoroscopic view of Synchromed II pump Introduction • HIV-related sensory polyneuropathy represents the most common neurologic complication of HIV infection and reflects several distinct etiologies: • Direct HIV-induced nerve damage3 • Complications of opportunistic pathogens, e.g. CMV infection4 • Toxic neuropathy from highly-active antiretroviral therapy (HAART)5 • Management is limited to opioids, anticonvulsants, lidoderm, and capsaicin which may offer limited relief. • An interventional approach may be indicated for patients whose symptoms are refractory to other measures. Conclusion For patients with comorbidities such as hepatitis C that preclude chronic oral narcotic use, ITDD may be a safe, efficacious, and reasonable interventional alternative to manage intractable chronic pain. • Two same-sex partners with HIV and hepatitis C sought chronic opioids to manage HIV-related polyneuropathy. • They complained of severe back pain and bilateral lower extremity neuropathic pain interfering with daily activities. • Both initially refused interventional approaches and received 24 mg oral hydromorphone daily for several years. • Worsening gastroparesis and cirrhosis prompted their hepatologist to seek alternatives to oral opioids. • Both elected for ITDD after demonstrating an excellent response to an outpatient trial of intrathecal fentanyl. • Intraoperatively, a 14-gauge spinal needle was fluoroscopically guided into the intrathecal space at L2-L3. • A 72-cm Medtronic spinal catheter was advanced to T11-T12 and anchored to the interspinous ligament. • The catheter was tunneled subcutaneously to a 40-ml Synchromed II pump anchored to the abdominal fascia. • Infusion was initially programmed at 0.48 mg morphine daily, with weekly outpatient 10% titration as needed. References 1. Penn RD. J Neurosurg 1987;67:182-6. 2. Kirkpatrick AF. Anesthesiology 2000;93:1553-4. 3. Simpson DM. Neurol Clin 1992;10:685. 4. Kim YS. Clin Infect Dis 1993;17:32-7. 5. Morgello S. Arch Neurol 2004;61:546-51. 6. Tarkatow IJ. Am J Med 1971;50:313-6. 7. Kreek MJ. Ann Intern Med 1972;77:598-602. 8. Li Y. J Infect Dis 2007;196:719-30. 9. Kumar K. J Neurosurg 2002;97:803-10.