Download
1 / 29
630 likes | 3.75k Views
OSTEOTOMIES ABOUT THE KNEE. Rod Martin M.D. FRCS(C). Outline. Introduction Distal Femoral Osteotomy Proximal Osteotomies of the Tibia Closing wedge osteotomy Coventry Slocum HTO with jig & plate Barrel-vault osteotomy Opening wedge osteotomy. OSTEOTOMIES ABOUT THE KNEE.

E N D
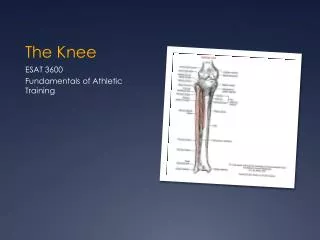
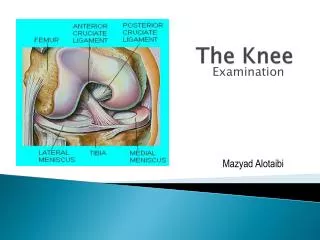
OSTEOTOMIES ABOUT THE KNEE Rod Martin M.D. FRCS(C)
Outline • Introduction • Distal Femoral Osteotomy • Proximal Osteotomies of the Tibia • Closing wedge osteotomy • Coventry • Slocum • HTO with jig & plate • Barrel-vault osteotomy • Opening wedge osteotomy
OSTEOTOMIES ABOUT THE KNEE • Patients with malalignment and unicompartment disease • Varus(4X) & valgus(5X) OA • 2020 OA will have largest increase of new cases of any disease • Unicompartment OA 30-60 age group • High demand / middle aged athlete
Indications Valgus deformity > 12 to 15 degrees Plane of the knee deviates from the horizontal >10 degrees 25-22 Varus Distal Femoral Osteotomy
Distal Femoral Osteotomy • Reported success 71% - 86% • Poor results with RA • Satisfactory results with TKR 94% • (13 of 18 had complications) • Difficulty restoring desired 5-10 degrees valgus
Coventry Medial or midline incision Rectus/medialis interval Insert blade at templated angle Osteotomy of femur Close wedge/secure plate 25-23 Coventry Distal Femoral Osteotomy
Proximal Osteotomies of the Tibia • Treatment of unicompartmental OA • 80% satisfactory results @ 5 years • Varus deformity = medial OA • Valgus deformity = lateral OA • Osteotomy “unloads” the “overloaded”
Proximal Osteotomies of the Tibia • Coventry (1965) • Medial closing wedge for valgus deformity • Lateral closing wedge for varus deformity • Advantages • Near the deformity • Cancellous bone heals quickly • Fragments held firmly by 1-2 staples • Permits evaluation of the knee through the same incision
Proximal Osteotomies of the Tibia • Coventry (1979) • 80% at 5 years & 60% at 10 years (213 knees) • Recurrence of deformity = recurrence of pain • Minimum “overcorrection” 8 degrees valgus • >30% ideal body weight = high failure
Proximal Osteotomies of the Tibia • Indications • Pain and disability • Unicompartment OA • Ability to use crutches post-op • Good vascular status
Proximal Osteotomies of the Tibia • Contraindications • Narrowing of lateral compartment • Lateral tibial subluxation of > 1 cm • Medial compartment bone loss > 2-3 mm • Flexion contracture > 15 degrees • Knee flection < 90 degrees • Correction of > 10-15 degrees • Inflammatory arthropathies
Proximal Osteotomies of the Tibia • Coventry correction formula • (1) Normal valgus (5-8 degrees) • (2) + amount of varus deformity • (3) + “overcorrection factor” of 3 to 5 degrees = total correction required (approx. 1 mm / degree)
Proximal Osteotomies of the Tibia • Maquet (barrel-vault) osteotomy • Inherently stable • “extensive” degrees of correction possible • Technically difficult • Intraarticular fracture • Scarring about the patellofemoral mechanism
Proximal Osteotomies of the Tibia • Medial opening wedge osteotomy • Does not “shorten” the extremity • Correct medial laxity • Surgery directed to the diseased compartment • Corrects up to 15˚
conclusions • Delays/avoids arthroplasty • Refute claims osteotomies compromise arthroplasty • Second “wave” of osteotomies coming
6mos post op Resumed all adl’s “knee feels 75% better”